
Introduction
Previous articles describe the development from prehistory to the end of the Viking period, of a cycle whereby increasing trade necessitated larger and more efficient ships to transport merchandise and better weapons to defend or attack, both of which facilitated more trading opportunities.1,2,3,4,5 However, it was not until the 18th century that Western medicine had sufficiently developed for this cycle to be recognised, thereby making possible the European settlement of Australia.6
While the technical developments in ships, weapons and medicine often developed independently in multiple regions worldwide, they remained closely linked throughout Western history in particular. This article continues this series by updating a previous two-part paper regarding the developments in ships, warfare and medicine during the English Tudor period from 1485 to 1603.7,8
Tudor ships
The previous article in this series describes how the post-Viking ‘knorrs’ (also ‘knarrs’) had evolved into ‘cogs’ and then ‘carracks’ by 1400. By 1500, these were three- or four-masted, with at least two square sails on the fore- and mainmasts, and fore-and-aft ‘lateen’ sails on the aft mast(s) to balance the sail plan and assist heading upwind. Their hulls were carvel-built, with a central rudder, integrated fore- and-aft ‘castles’ and an ’orlop’ deck below the ‘main’ or weather deck. Many could stow sufficient crew supplies and cargo to either make viable commercial voyages worldwide or transport large numbers of troops and their stores over shorter distances.
This allowed carracks to displace the smaller, faster and more manoeuvrable ‘caravels’ used by Portugal from 1415 to trade with West Africa, and then bypass the Venetian and Genoese dominance of the Mediterranean trade routes to India and China. To this end, Bartholomew Diaz reached the Cape of Good Hope in 1487,9 followed by Vasco da Gama reaching India in 1498.10 Meanwhile, in 1492, the Spanish monarchy gave Christopher Columbus three ships to find another route to China by sailing west (only to discover America),11 while Ferdinand Magellan used five ships for his 1519–22 world circumnavigation.12 Magellan was followed by explorers such as Alvaro de Mendana, who discovered the Solomon Islands in 1568 (followed by a failed colonisation in 1595), and Pedro Fernandes de Queiros in 1605–06, whose search for Terra Australis led to Luis Vaz de Torres passing Cape York in northern Australia.13
Hence by 1600, Portugal, Spain, England, Holland and France had ships that were technologically capable of voyaging anywhere worldwide in search of colonies, trade and/or plunder. These enabled the Spanish colonisation of central and south America, the Philippines and Portuguese colonies in modern Brazil, Africa, India and the East Indies. The following century saw Portugal lose most of the East Indies to the Dutch, and England and France take some of Spain’s Caribbean colonies while establishing new colonies in northeast America. However, the developments in seagoing sanitation, victualling, water quality, ventilation, personal hygiene and conditions of service necessary to reliably keep the crews alive that made these events possible, lagged behind until after the 1740s.

Figure 1. Replica carrack c.1500, Vila do Conde, Portugal.14 Note the carvel-built hull, three masts each with yards for one or more sails, integral bow and stern castles, and no gunports.

Figure 2. Replica caravel Boa Esperança used by Bartholomew Diaz to round the Cape of Good Hope in 1488.15 Note the finer hull and fore-and-aft lateen sails.
The previous article describes how, besides their use for crew accommodation, the carracks’ fore- and-aft castles also provided a height advantage for their crews to defend against or conduct peacetime piracy, or for soldiers to fight from in wartime. Although sea battles were still mostly fought with blade- and torsion-type weapons, these were slowly being displaced by handheld firearms. At the same time, the weight of crew-served ‘great guns’ meant very few could be carried on their weather decks without compromising stability. Hence, like their cog predecessors, carracks were used interchangeably for warlike and peacetime purposes.
Henry VIII therefore initiated a naval revolution when he commissioned the Mary Rose in 1511. Following her capsize off Portsmouth in the Solent in 1545 and salvage in 1982, the surviving hull structure comprises a half-section from bow to stern, with the port side missing. The lowermost level was the hold, containing ballast, stores and a brick galley. Above the hold was the orlop deck, which contained more stores and equipment such as longbows and other hand weapons. The main deck above the orlop had gunports for at least seven ‘great guns’ per side, and four surviving cabins including one for a barber-surgeon. The weather or upper deck had more ‘great guns’, smaller anti-personnel guns and archers shooting behind protective blinds under anti-boarding netting.16
As the first ship with hull gunports, the Mary Rose carried more and larger ‘great guns’, thereby making grappling and boarding more difficult. This initiated the eventual elimination of soldiers as the ship’s primary armament in favour of more sailors, which also facilitated better ship handling.17 As this also rendered height advantages moot, English carracks had evolved into ‘race-built’ galleons by the 1570s, with lowered fore-and-aft castles on longer and narrower hulls enhancing their speed and manoeuvrability. Hence, although all ships still had to defend themselves, galleons begat the differentiation in Europe between bespoke warships and merchantmen.18,19

Figure 3. Henry VIII’s Mary Rose, c.1520.20 Note the bluff carrack hull with high (two-storey) fore-and-aft castle, four masts, the anti-boarding nets and (in particular) the hull gunports
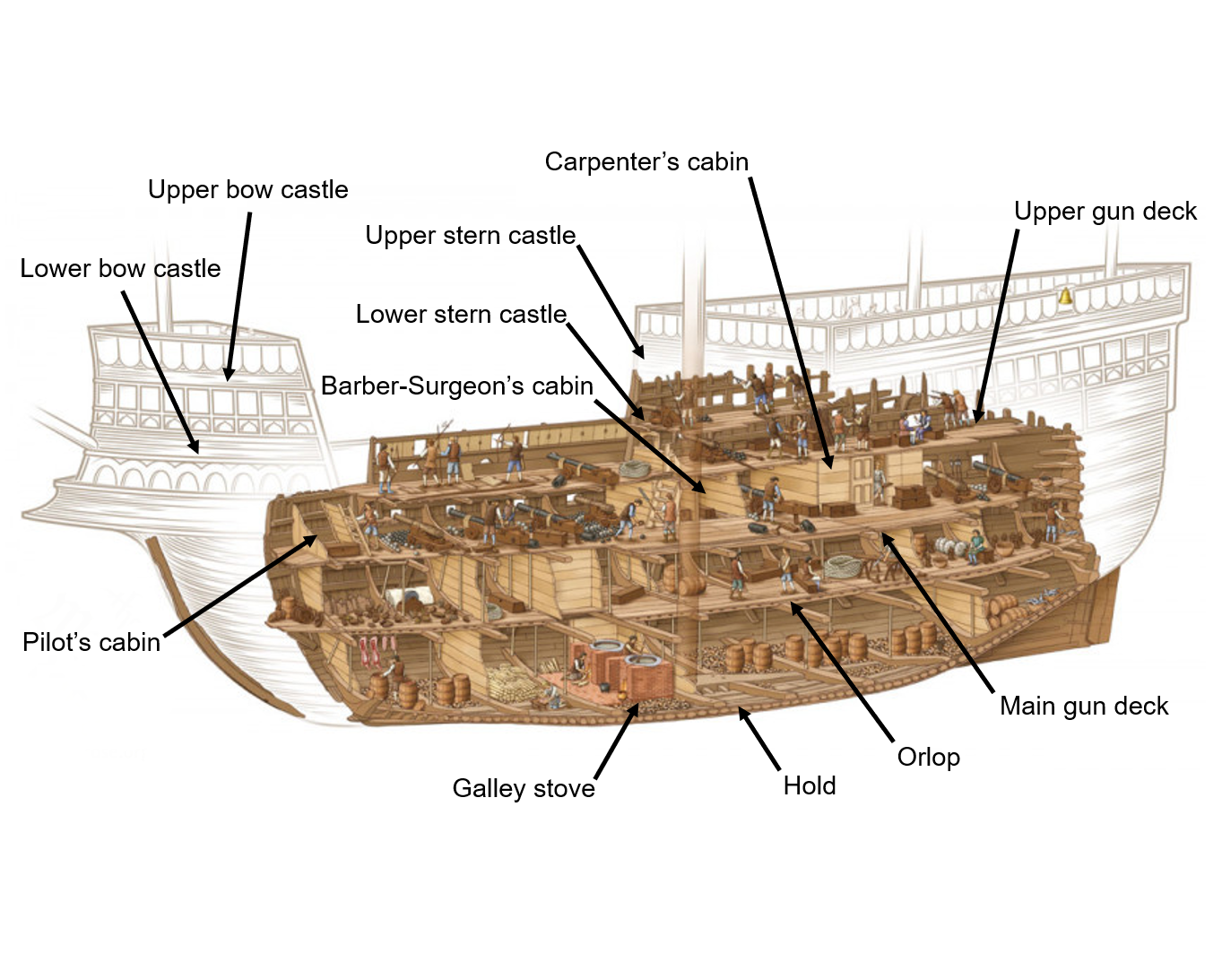
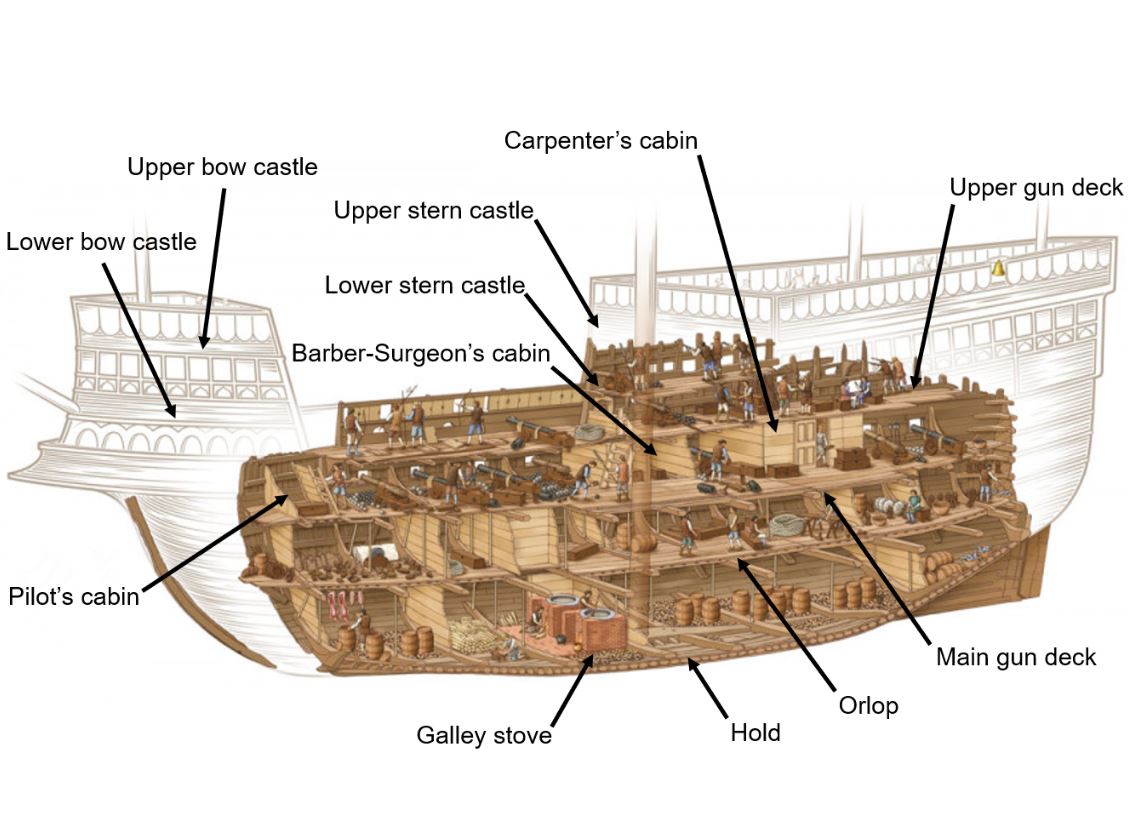
Figure 4. Henry VIII’s Mary Rose post-salvage isometric diagram.21

Figure 5. Francis Drake’s Golden Hind c.1577.22 Note the longer and narrower ‘race-built’ galleon hull, lowered (single-story) fore-and-aft castles, gunports…and her small size.
Tudor naval medicine
Physicians and surgeons
The previous article described how English medieval medicine gradually aligned with the Galenic model used by the rest of western Europe.23,24 Although the Royal College of Physicians of London was not established until 1518, the relationship between university-educated physicians and apprenticeship- trained apothecaries already entailed a select group of the former catering to the nobility who could afford them while supervising the latter selling their wares to the masses.25 On the other hand, after a somewhat precarious existence since its founding in 1363, the Fellowship of Surgeons that was intended likewise to supervise barber-surgeons, was subsumed into the London Barber-Surgeons Company in 1540.26
The ensuing split in the English medical profession led to numerous naval disasters over the next three centuries: the physicians’ higher social status meant they rarely went to sea, while ‘sea-surgeons’ lacked the legal authority and expertise to manage the medical cases that comprised most of their clinical workload.27 The fact that surgeons began their careers as apprentices also led to confusion regarding their roles. Despite having been separated within the same company since 1376, barbers could still perform ‘procedures’ such as trimming corns, while sea-surgeons had to obtain barber’s tools and learn how to use them.28
Even so, further shipboard technical improvements led to incidental health benefits. Better bilge pumps had already enabled drier and hence healthier ships, while in 1578, Sir William Wynter advocated large stone ballast rather than gravel to help keep ships’ holds clean (although the French continued to bury their dead in their ships’ ballast until the 18th century).29,30 The French introduced hammocks for bedding in the 1550s, with Sir Walter Raleigh driving their use in English ships from 1597.31 In 1590, Sir John Hawkins followed Wynter’s suggestion to move his ship’s galley from the hold to the upper deck, thereby reducing food contamination from bilge water.32 However, sanitary arrangements comprised ‘necessary seats’ over the ship’s bow, while tubs were used below deck—albeit not always by passengers or troops—as combined urinals and fire buckets.33
This combination of technological advances and a split medical profession meant seagoing living conditions were controlled by ship’s captains, whose authority and practical experience meant they were often met with some success. From there, it was only a small step for them to take over all non-surgical health issues, leaving the surgeons with only the actual hands-on application of their skills. In 1519, surgeon Thomas Roos wrote that these included controlling haemorrhage, trephining, couching for cataract, removing sequestra, suturing wounds, lancing abscesses, reducing fractures and dislocations, dental extractions and bloodletting.34
Some of these skills were acquired via the four executed criminals received annually by the London Barber-Surgeons for dissection purposes from 1540. However, most surgeons’ medical education came from books by authors such as Thomas Vicary (c1490–1561) and Thomas Gale (1507–1587).35 The true father of English naval medicine, however, is William Clowes (1544–1604), who wrote A Prooved Practise for all Young Chirugeons in 1588, which he updated in 1596 into A profitable and Necessarie Booke of Observations for all Those that are Burned with the Flame of Gun Powder, and also for Curing of Wounds made with Musket and Caliver shot, etc. Having qualified at age 19, Clowes served at sea for several years. In 1570, he treated a boatswain with two fractured ribs aboard the 200-ton Aid (half the size of a modern Cape-class patrol boat) by removing a bone sliver abrading the pleura. He also recognised the primary and secondary stages of syphilis as the only time it could be treated using an external application of mercury, and even associated scurvy with the seamen’s diet. For below-knee amputations, Clowes used an operating table on which an assistant sat astride the patient holding both arms down, another astride to secure the thigh and a third to hold the distal limb. He used a tourniquet for both haemorrhage control and analgesia; as it was released, he found and stopped each bleeder, a technique that, with adding four cross sutures to cover the stump, was used at sea for the next three centuries.36
The Mary Rose medicine chest
Clowes also advised his students on what a medicine chest should contain, using his own as a model. This was probably similar to one retrieved from the Mary Rose in 1980, which was made of walnut with dovetailed corner joints, with a solid bar pierced for rope handles at each end. Measuring 1330 x 485 x 460 mm, it has no internal partitions apart from a shallow lidded shelf on one side. The 64 objects within included eight wooden containers of ointments and another containing peppercorns. One had a resinous substance that may have been frankincense, complete with scoop marks from the surgeon’s fingers. The chest also had five ceramic jars that may have contained linseed oil, resins, henbane, quince or belladonna. Other contents included a pewter bleeding bowl, a small brazier for warming a chafing dish, a mortar for grinding drugs and several sausage-like rolls of unguents, made with a 2:1 ratio of Fuller’s earth and frankincense that may have been used as plasters.
The chest also had a brass and a pewter syringe, with small rounded nipples at their needle tips. Ambrose Paré (1510–90) referred to using small urethral syringes for bladder stones and gonorrhoeal strictures and ‘glisters’ or large syringes for the ‘flux’ (diarrhoea) and constipation. It had also had surgical instruments: although their blades had corroded away, eight handles were found similar to 17th-century cauteries, with a larger handle that may have been part of a large knife or amputation saw. Consistent with the surgeon also being the ship’s barber, there were eight cut-throat razors, a brass shaving bowl and a whetstone. Apart from the chest, his cabin had additional wooden and glass containers, a low wooden bench that may have been used for applying plasters, and personal possessions, including pewter plates, wooden bowls, shoes and a purse of silver coins. A highlight was his coif, a hat made of fine silk velvet. Even so, the fact that he had two combs (within and without the chest), indicates even he was not immune from acquiring his own tonsorial livestock.37

Figure 6: Mary Rose barber-surgeon’s chest and a selection of contents.38
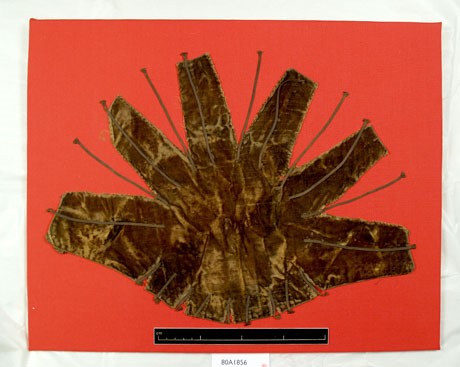
Figure 7. Mary Rose barber-surgeon’s coif, made of black velvet.39

Figure 8. Painting by Hans Holbein the Younger (1497–1543), commemorating Henry VIII’s 1540 Royal Charter to the London Barber-Surgeon’s Company.40 Note the barber-surgeon’s headwear.
Hospitals
The previous article noted that, notwithstanding the secularisation of medical practitioners from the 13th century, accommodation for the English sick and disabled was provided by up to 800 monasteries through their ‘houses of pity’ and bespoke sailors’ ‘masyndews’.41,42 However, the Wars of the Roses (1455–1485) led to a period of economic disruption that rendered many smaller monasteries financially non-viable, which was followed by their dissolution by Henry VIII in 1536. As this forced the closure of nearly all ‘houses of pity’, including the masyndews, parishes began funding secular hospitals from the 1550s, supplemented by the privy purse, levies (such as those on ships entering Bristol for the local mariner’s hospital) and lay benefactors such as Sir John Hawkins, who provided a ten-bed mariner’s hospital at Chatham in 1594. However, it was only from 1597, when benefactors like Hawkins could make such donations without royal approval, that these hospitals provided even the limited medical care previously offered by the monasteries.43,44
Meanwhile, permanently disabled mariners depended on begging licences, or competed with other sick and poor for whatever charitable accommodation remained. This was until the medical aftermath of the 1588 Armada campaign led Lord Howard, Sir Francis Drake and Hawkins to organise the Chatham Chest in 1590. This was an independent mutual benevolent fund to which every seaman in the royal ships contributed sixpence a month, usually in exchange for a one-off payout rather than a pension. Despite multiple embezzlement scandals, the Chest endured until its merger with the Greenwich Hospital naval pensioner scheme (introduced in 1691) in 1814.45
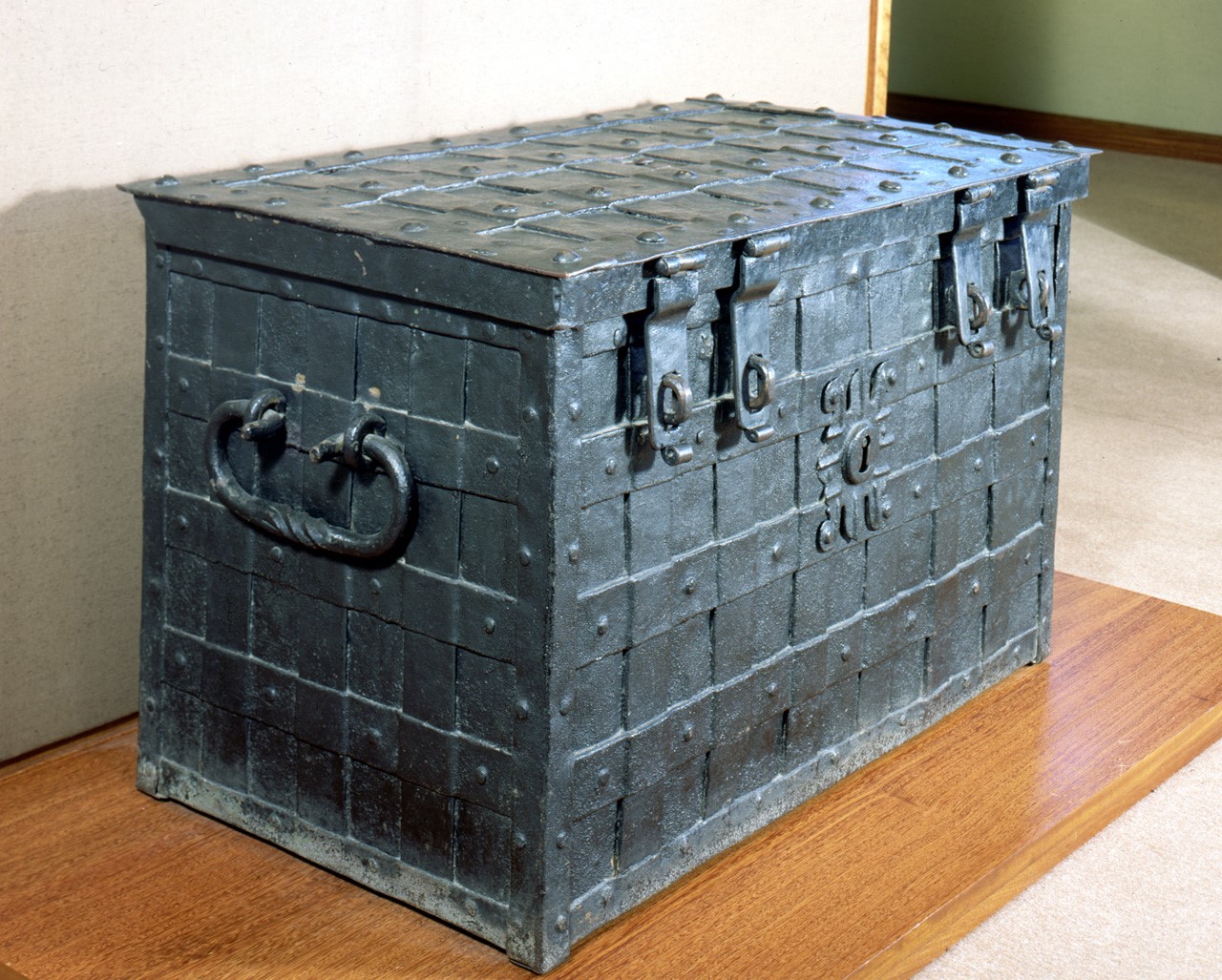
Figure 9. The original Chatham Chest, built c.1625.46 Note the false central lock (the actual lock is in the lid) and four padlock hasps, the keys to which were putatively held by different people.
Hence, the Tudor wars were fought with minimal medical care for anyone, let alone sailors. Human remains from 179 individuals from the Mary Rose (including 92 fairly complete skeletons) indicate they were primarily aged in their late teens and early twenties with an average height of about 171 cm. Many adult teeth had enamel hypoplasia indicating previous malnutrition, consistent with a famine during the winter of 1527–28. Other findings included rickets, scurvy, anaemia, non-reduced fractures, avulsion injuries and osteoarthritis. Given the restrictions on removing clothing at sea, the 81 combs suggest less-than-ideal hygiene standards— all except two were made of boxwood, double-sided and fine-toothed, indicating their use for delousing.47 Even so, direct evidence of infectious disease was limited to tuberculosis.48
A separate finding was a 12.5% incidence of mostly left-sided os acromiale (non-union of the acromial epiphysis), compared to a modern incidence of only 3–6%. One possible reason relates to Henry VIII enforcing a 14th-century law that all fit males from 7 to 60 practice using the longbow. Tests of 172 bows from the Mary Rose indicate that they had draw forces of 50 to 75kg, compared to 20kg for modern bows. As longbows are also drawn differently (for a right-hander: extending the left arm and shoulder rather than flexing the right), the technique may have been responsible in addition to the forces involved.49
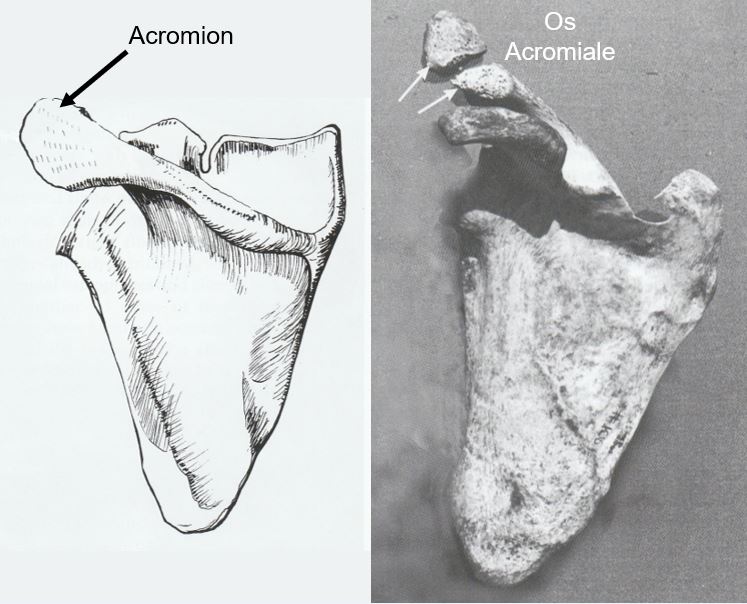
Figure 10. Right scapula with a normal acromion (left), and one from a Mary Rose crewman with os acromiale (right)50

Figure 11. Re-enactor Mary Rose archer with a replica longbow.51 Note the strain on both shoulders (especially on the left used to draw the bow rather than the right).
Tudor naval warfare
Before the Armada
The first known disease outbreak to influence an English naval campaign occurred in 1544, when a French fleet was defeated, not by Henry VIII’s ships but by food poisoning. Besides losing the Mary Rose the following year, another 11 of his ships sustained a ‘bloody flux’ (diarrhoea) that killed a quarter of his 12 000 men in 10 days.52 In 1553, Sir Hugh Willoughby took three ships and 63 men in search of a route to China via northern Russia, with only one making it to Archangel. Having been frozen in off Lapland, the other ships were found the following spring with no survivors from starvation, scurvy, exposure and possible carbon monoxide poisoning.53 The same year, Thomas Wyndham’s expedition to Benin in West Africa lost 100 men out of 140 to yellow fever.54,55
The Anglo-Spanish war from 1585 followed 20 years of English interference with Spain’s colonial trade, not only for plunder but also to deny funding for its wars against the Netherlands.56 As her own fleet lacked the numbers, Elizabeth I’s maritime power was based on privateers, beginning in 1562 when John Hawkins carried manufactured goods to West Africa, slaves to America (the infamous ‘middle passage’) and agricultural products back to England. This ‘triangular trade’ contributed significantly to English prosperity (and the naval power that defended it) over the next 250 years. Even so, although Hawkins’ first voyage was disease-free and only 20 crew were lost on the next in 1564, his third in 1568 ended in disaster when he and his kinsman, Francis Drake, were ambushed in the West Indies.57 This led Drake to carry surgeons on his later voyages, who proved their worth when he was wounded in 1572 while raiding the Caribbean.58
In December 1577, Drake left England with 164 men in five ships to raid the Pacific. Having passed through the Straits of Magellan, his ship Golden Hind was alone and her master surgeon had died, while his mate was no more than ‘a boy, whose goodwill was more than any skill he had’. Hence, Drake himself had to treat nine wounded men despite having been grazed under the eye by an arrow. By obtaining fresh supplies while looting Spanish America, Drake kept 85 men fit until he reached California in April 1579. On abandoning a search for a Northeast Passage back to England, he returned home via the Moluccas in September 1580 with 59 survivors.59.60
The first English expedition to the East Indies and China via the Cape of Good Hope left in 1582, but returned the following year, having failed to leave the Atlantic. Its surgeons included the future lecturer, anatomist and (highly unusually) physician John Banester (1540–1610), who lost 45 of 135 men, of whom only three were surgical cases.61 In 1585, Elizabeth lent six ships to Drake to raid the West Indies with 2400 men. He lost 300 from malaria raiding the Cape Verde Islands and another 500 by taking the mosquitoes with him to Dominica, the epidemic only ending in the colder latitudes on the way home.62,63 On the other hand, Thomas Cavendish left for the Pacific the same year with three ships and 123 men. He lost only one man in action (shot by an arrow, of which only the shaft was removed as he refused to have the head removed), two from scurvy and one from possible dengue, before his two surviving ships arrived home in September 1588.64,65
The Armada campaign
The Armada campaign began when Drake attacked the Armada’s base at Cadiz in 1587, thereby delaying its sailing that year.66 Elizabeth’s reliance on privateers meant that 83% of her 197 Armada ships were either privately owned warships or armed merchantmen.67 Most were ‘race-built’, with half of their 16 000 men being both seamen and gunners, thereby enabling new tactics based on long-range gunfire rather than boarding.68 By comparison, the Armada had 130 ships, including 25 purpose- built warships of the ‘high-charged’ type to facilitate boarding. They carried 30 000 men, organised similarly to land fortresses with bespoke soldiers, gunners and sailors. As the latter only comprised 8000 men, these ships were overcrowded yet had too few seamen to be handled effectively.69
The Armada crisis overtook an England enfeebled by years of poverty and malnutrition. No processes existed for recording or disseminating the preventive health lessons learned from the 1544–45 or 1558 campaigns, while the Divine Right of the sovereign meant any attempt to apply instructions not directly emanating from the Crown was considered treasonous.70 Embarked landsmen failed to comply with the basic hygiene standards now accepted by experienced seamen, none were allowed to undress on board and no clothing was supplied, allowing lice and fleas (hence typhus) on board.71 Even so, it was the victualling that created an English medical catastrophe even before the Armada left Spain, with dysentery and toxic food poisoning taking their toll after as little as a fortnight at sea. For example, the Elizabeth Jonas lost 200 out of 500 men in three weeks in Plymouth; on sending the survivors ashore and replacing her ballast, she lost even more during the Armada pursuit. Although the Privy Council asked the College of Physicians to send four physicians to the fleet, they achieved little, and, rather than the victuals, they ascribed the outbreak to the beer (drunk instead of water as it kept better).72
Although it was ready to depart Lisbon on 25 April, the Armada did not get to sea until 30 May, whereupon bad weather and an inability to beat upwind meant it did not enter the English Channel until 19 July. This delay combined with poor food preservation meant their victuals likewise decomposed, but without resupply. Water was limited to three pints per man per day, even before many casks were found empty or leaking. The soldiers were kept below in overcrowded typhus-spreading conditions, while the rough weather led to their vomit and excreta washing over their rotting food and tainted water into the bilges. The resulting effluvia was only pumped out as far as the upper decks, where it either found its way overboard or recycled itself back below.73
The following week saw a series of running battles up the Channel, during which the English long-range gunnery tactics initially proved indecisive, apart from preventing the Spanish from either boarding their ships or landing troops ashore. Only after the Armada’s cohesion was disrupted by a fireship attack on 28 July off Calais, did they find short- range gunfire more effective. On running out of ammunition, the English left the Armada to its fate on 13 August off the Firth of Forth, having lost no ships and less than 100 men in action.74 However, as they dispersed to the east coast ports, their administrative system broke down completely, while their own typhus epidemic revealed the limitations of the Laws of Oléron in finding enough accommodation for large casualty numbers since the demise of the ‘houses of pity’ and masyndews.75
Meanwhile, the Spanish had 3000 typhus cases in addition to their wounded. Even in the best- provisioned ships, three or four men were dying daily from starvation and thirst. Many ships disintegrated in the north Atlantic autumn without survivors, and at least 26 were wrecked on the Irish and Scottish coasts. In total, up to half of the Spanish ships never returned, and about 20 000 men died, comprising 1500 killed in action, 6000 shipwrecked or lost at sea, 1000 murdered after shipwreck and the remainder by starvation and disease.76

Figure 12. Battle of Gravelines, 29 July 1588.77Although alliterative, this depiction shows the battle being fought in multiple melee-type actions.
After the Armada
In 1589, Drake led a ‘counter-Armada’ to attack Spain via Lisbon with 140 ships and 13 500 men. After another victualling debacle resulted in its abandonment, he cruised between the Azores and Vigo before returning to Plymouth with little accomplished, having lost half his men from disease. The £253 allocated for medical supplies had proved inadequate, as was the surgeons’ experience and expertise.78,79
In 1591, James Lancaster left for the East Indies in three ships and 200 men, returning in 1594 via the West Indies with no ships and only 25 survivors. His next voyage in 1594–95, with 275 men in three ships, was more successful, capturing 29 ships and holding Recife (in modern Brazil) for a month.80,81 Both voyages well-prepared Lancaster for his next voyage in 1601, the first by the new English East India Company.
Meanwhile, in 1591, the Spanish caught an English fleet under Lord Howard off the Azores with half his men sick after yet another victualling failure. Having off Sir Richard Grenville’s Revenge, she held off the Spanish for 15 hours despite having 90 of her 190 men ill in her hold, killing 400 to 1000 men in exchange for 40 killed and most of the rest wounded before exhausting her ammunition. On surrendering, Revenge’s hold flooded, drowning her sick, and she sank in a storm with all her survivors and prize crew.82,83
Cavendish’s second voyage to the Pacific in 1591 with five ships and 76 men was less lucky than his first, with scurvy killing him and 48 men before they reached the Straits of Magellan. Having recovered by eating ‘scurvy-grass’ and penguins, another 11 died on the way home (possibly from ‘wet’ beriberi), and, with only five men fit to work the last remaining ship, she was run ashore on arrival.84,85
In 1593, John Hawkins’ son, Richard, sailed for the Pacific with three ships. Scurvy developed near the equator, and despite having seen ‘10 000 men with this disease’ and recognising the value of fruit juice as a cure, he failed to link the two amid a plethora of other theories, such as the sea air, having a dirty ship and lack of exercise. By the time he reached Brazil, rats had eaten 80% of his victuals and he only had 24 fit men. Nevertheless, his crew recovered with oranges and lemons and remained well until they met two Spanish ships off Chile, where they surrendered after a two-day battle. Despite missing most of their instruments, English surgeons lost none of their own 40 wounded and even treated the Spanish casualties after their surgeons proved incompetent.86 This was probably the first time naval surgeons made a positive difference in battle casualty care.87
Like scurvy and fresh food, the link between dysentery and water quality was missed for centuries. This was evident when Drake and John Hawkins left Plymouth for the West Indies with 21 ships and 2500 men in August 1595. The medical preparations appear to have been very good, with surgeon James Wood, several assistants and medical chests, slop (spare) clothing and advice from Hugh Platt (1552–1608) regarding water and other stores. Years later, Platt wrote Certaine Philisophical preparations of Foode and Beuerage for Sea-men, in Their Long Voyages, which anticipated the development of tinned food 200 years later, and suggested macaroni as a cheap, fresh and lasting staple for use at sea.88 However, John Hawkins died off Puerto Rico om 12 November, followed by Wood and then Drake on 28 January 1596. By 6 February, another 500 men had joined them, and the survivors sailed home after scuttling some ships to man the rest.89 While another 1595 expedition to raid the Canary Islands and capture Puerto Rico was likewise forced back home by ‘a bloody flux and other distempers’, a second attack on Cadiz the following year was moderately successful, with no illness and only a few wounded .90,91,92
Elizabeth’s 1600 Royal Charter to the East India Company begat the corporatisation of England’s transoceanic trade. Its first expedition, led by Lancaster, comprised 480 men in five well-found ships, each with a barber and two surgeons, the latter receiving allowances of between £20 and £32 for their chests. Even so, his success in establishing ‘factories’ in Sumatra and Java cost over half his men dead from disease by the time he arrived home in mid-1603. Yet, despite over 100 scurvy deaths across his ships, he kept his own relatively scurvy-free by issuing his men three teaspoons of lemon juice daily. Hence, although this success was again lost (as was his linking dysentery with water quality), Lancaster is credited as the first seaman to use lemons to prevent scurvy.93
As the Company fought the Portuguese and Dutch for the East Indian markets, it became policy for its ships to carry a surgeon and a mate, whose provision by the London Barber-Surgeons soon became just as important a role as doing likewise for the navy and army. In requiring its surgeons to write journals to develop a scale of medical equipment for use at sea, it was the ‘John Company’ rather than the navy that soon became England’s central repository for nautical medical knowledge.94
Conclusion
The disruption of the English social order and the demise of the religious orders destroyed many of the rudimentary health institutions that existed at the end of the Middle Ages. Ironically, the demand for them increased as English sailors ventured overseas.
Tudor overseas trade was fraught with health risks, both at sea and ashore. The seeds for destruction from scurvy, typhus and dysentery were often sown even before the ships left England, resulting from poor victualling and worse hygiene practices. Even if these had been better, little could probably be done regarding diseases that wreaked so much havoc, such as yellow fever and malaria, given the inability to differentiate, let alone diagnose them. There was also a lack of natural immunity to illnesses imported from overseas, although indigenous peoples exposed to diseases exported from Europe did even worse.
Furthermore, sea-surgeons existed only to treat wounds rather than illness and were further hamstrung by legal constraints on their training, which actively prohibited their acquiring any expertise in internal medicine. Even if this had been otherwise, the level of therapeutic support was often limited to hiding rather than treating the cause. In any case, the physicians’ reliance on humoral medicine further militated against their effectiveness. As a result, it is hardly surprising that mortality rates sometimes reached almost universal proportions. Although connections had been made between diet and scurvy, water quality and dysentery, and mosquitoes and malaria, these were lost not once but several times over the next 200 years, caused by a lack of peer support and a naval medical administrative system to record and promulgate them.
The story of Tudor naval medicine is therefore one of multiple disasters among occasional successes, the latter including Cavendish’s 1585–88 circumnavigation and Richard Hawkins’ post-action casualty care in 1593. Since the period essentially defined the medical problems associated with going to sea, it would be up to their successors (seaman and medical) to develop the solutions.
Disclaimer
The views expressed in this article are the author’s and do not necessarily reflect those of the RAN or any other organisations mentioned.
Corresponding Author: N. Westphalen, neil.westphalen@bigpond.com
Authors: N. Westphalen1,2
Author Affiliations:
1 Royal Australian Navy – Directorate of Navy Health
2 University of New South Wales Canberra at ADFA



