
Introduction
Previous articles describe the development from prehistory to the end of the Viking period, of a cycle whereby increasing trade necessitated larger and more efficient ships to transport merchandise and better weapons to defend or attack them, both of which facilitated more trading opportunities.
However, it was not until the mid-18th century that Western medicine had sufficiently developed for its role as an operational enabler of this cycle to be recognised, which, among other things, made possible the European settlement of Australia.
While the technical developments in ships, weapons and medicine driven by this cycle often developed independently in multiple regions worldwide, they remained closely linked throughout Western history. This article updates a previous paper that describes some of the technical and other developments in ships, warfare and medicine during the English medieval period between 1200 and 1500.
Medieval ships
By the end of the Viking period, Northern European ships mostly comprised ‘knorrs’ (also ‘knarrs’). These were essentially large open boats, with overlappingedge or ‘clinker-built’ hulls that were shorter, rounder and progressively less amenable to being rowed compared to their Viking longship predecessors, and a single mast with a single square sail. Lacking permanent cabins, any crew and passenger shelter was made of canvas, while hot food would have been prepared—if and when the need arose—over a wood fire on an open deck. Although their seaworthiness, combined with the European introduction of the navigation compass sometime before 1190, would have allowed them to undertake limited voyages offshore, their susceptibility to being swamped and sunk meant knorrs routinely undertook brief coastal passages only during the northern summer months.
However, increasing trade required larger ships, which led to knorrs becoming ‘cogs’. These had centre-line rudders instead of steering oars, which improved their manoeuvrability and allowed them to come alongside on the ‘steerboard’ side of the ship as well as the ‘port’. Cogs also had hulls deep enough to need weather decks to work the ship, which, besides reducing their risk of being swamped, created space below for crew and passenger accommodation and cargo. Besides making living conditions slightly less arduous, these developments made cogs safer and more profitable in peacetime while also allowing them to carry more troops and supplies in war.
Even so, their small size continued to limit their winter operations. At the same time, the absence of efficient bilge pumps not only still made for wet living conditions below but also increased the hygiene hazards posed by stagnant seawater, decomposing food waste and spilled perishable cargo, rats and their droppings, and sewage from passengers or troops relieving themselves below rather than on deck in bad weather. Although a prohibition on undressing at sea further exacerbated these hazards,12 they were partly mitigated by the cog’s endurance remaining limited to, at most, a few days.
By 1285, cogs had also acquired temporary wartime fore-and-aft ‘castles’, which gave soldiers a height advantage to either grapple and board or defend against such attacks. These castles were permanently integrated into the cog’s structure from about 1350, allowing their crews to use them to defend against (or partake in) peacetime piracy. The space below the castle decks came to be used for crew accommodation (sailors forward, officers aft), freeing the hold below the weather deck for additional passengers and cargo or troops and stores.
As the northern powers extended their trade into the Mediterranean, their crews were exposed to local shipbuilding traditions that greatly influenced their own. By 1400, larger cogs had acquired two or more masts, thereby becoming ‘carracks’. Over the next century, the single large square sail on each mast was displaced by two or more easier-to-handle sails, with additional fore-and-aft ‘lateen’ sails at the ship’s rear to balance the sail plan, and assist heading upwind. As carracks themselves increased in size, the limitations of clinker-built hulls led to their carvel (edge-to-edge) construction. This resulted in ships large enough to acquire a second ‘lower’ deck below the weather or ‘upper’ deck, thereby freeing the hold for cargo except for the galley or ‘cookroom’ amid the aforementioned effluvia that remained despite the first effective bilge pumps.
Hence by 1450, northern European carracks could remain at sea in most weathers over weeks or months, with enough passenger and cargo-carrying capacity to make longer voyages profitable. These capabilities initiated an era of exploration over the next three centuries to pursue opportunities for worldwide trading (and later colonisation). However, although they had sufficient clientele to justify seagoing surgeons—especially when carrying troops—and (just) enough room for them to work on board, the concomitant advances in personal and shipboard hygiene, food and water preservation, clothing, ventilation and other attributes necessary to prevent disease—not only as an end unto itself but to also facilitate trade opportunities—were not achieved until after the 1740s.
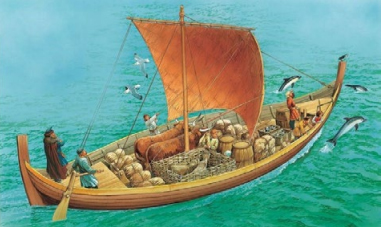
Knorr, c.1200. Note the clinker-built hull, steering oar, open deck without shelter and small crew size.
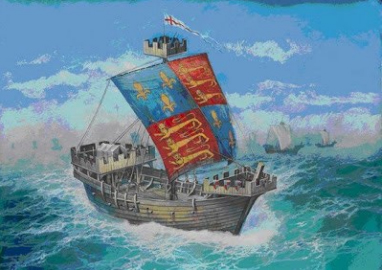
Representation of Edward III’s flagship Cog Thomas, which fought the Battle of Winchelsea on 29 August 1350. Note the clinker-built hull with central rudder, weather deck enclosing the hull, and non-integral fore-and-aft fighting castles. Her troops are omitted.
Carrack, c.1400. Note the carvel-built hull with integral fore and after castles, the additional stern fighting castle, two masts with an aft lateen sail, and greater crew size.

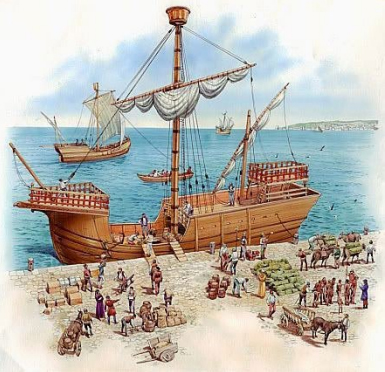
Replica carrack c.1500, Vila do Conde, Portugal. Note the carvel-built hull, three masts with yards for one or more sails, and integral bow and stern castles.
English medieval naval warfare
During the five centuries following the 1066 Norman conquest, the term ‘navy’ referred to all the ships that enabled English maritime power, whether owned by the monarch (if he had any) or his merchant subjects and was mostly limited to the Channel and the North Sea. Besides trading with continental Europe, they were used to transport armies and their stores to and from France, countering piracy and defending against invasion. Moreover, the monarch would hire his ships out to the merchants for trade and ‘arrest’ their ships and crews for his own purposes when required. In addition, the harbours at Dover, Hastings, Hythe, Romney and Sandwich (which remained the Cinque Ports despite the addition of Rye, Winchelsea and other towns from the 1190s) furnished the monarch with 1140 men and 57 ships for 15 days per year in exchange for certain tax privileges. 21 Furthermore, English ships were built in ad hoc locations rather than dedicated shipyards until the early 15th century. While a Clerk of the King’s Ships provided administrative support for all royal and ‘arrested’ ships from 1344, this typically entailed only managing the finances.
Hence, medieval English mariners performed their duties interchangeably between their monarch and private employers under the Laws (also Rules or Rolls) of Oléron. ‘Olroms’ originated as the Maritime Assizes of the Kingdom of Jerusalem, which were based on the ancient Lex Rhodia that had governed Mediterranean commerce for centuries prior to the Christian era. They were introduced to England by Henry II’s wife, Eleanor of Aquitaine, who brought the assizes from the Second Crusade and set up a maritime court on the Ile of Oléron to administer them sometime after 1160. On their incorporation into English law in 1190, they covered numerous matters, including the responsibilities of masters with respect to hiring their crew, profit shares, discipline and welfare.
As ‘Olroms’ applied to all English ships, irrespective of who owned them, shipboard ‘command’ was held by the same ‘master’ in both peace and war. These began their professional life as apprentices when the absence of charts or pilot guides meant their navigation skills, in particular, were dependent on memory.
As ships became larger and more complex, they required increasingly specialised crewmembers such as the boatswain, carpenter and cook, who were joined in the royal ships by the gunner, purser and, from 1510, the surgeon. Apart from the cook—whose job existed to keep disabled seamen employed and hence did not require any culinary expertise—their professional development was likewise based on long apprenticeships. The master’s role as a ‘first among equals’ per ‘Olroms’ meant there was no formal seagoing ‘officer class’ until the mathematicallybased navigation methods introduced in the mid16th century required better literacy skills. Although the prevalence of piracy meant that sailors often had to defend themselves even in peacetime (unless engaging in it themselves), soldiers were carried on the rare occasions that entailed serious battles.
These included an action off Dover in 1217 at the end of the First Baron’s War, and the battles of Sluys (modern Sluis) in 1340 and Les EspagnolsSur-Mer in 1350 during the Hundred Years War. These entailed the sailors getting their ships close enough for the embarked soldiers to attack with bows and lances until they could grapple and board, and then either holding alongside or breaking free of their opponent, depending on how the battle fared. Boarding led to melee hand-to-hand fighting with swords and axes while the opposition threw rocks and lumps of metal from the masthead tops. Neither side gave quarter, and the losers went over the side whether or not they were wounded.
These soldiers came under a military commander, who, in accordance with their feudal obligations to their monarch, came from the English aristocracy on the same terms as ashore. This usually also gave them command over the master and his crew, which they continued to exercise even after their soldiers were rendered redundant by large-calibre below-deck guns after 1500.
Hence, by the mid16th century, English royal ships had evolved two types of officer: ‘gentlemen’ who were ‘commissioned’ to exercise command on the monarch’s behalf, and ‘tarpaulins’, who received ‘warrants’ from the Navy Board introduced by Henry VIII in 1546. The
latter included naval surgeons, who did not have commissioned status until 1843.
The first English ship known to carry guns was the Christopher of the Tower in 1338. She had three iron guns and a handgun, which were mounted on the fore and after castles as anti-personnel rather than anti-ship weapons.
It was not until after 1410 that Henry IV began mounting large numbers of such guns aboard his ships, while his son, Henry V, built larger and stronger ships (including the world’s first three-masted carrack Grace Dieu) with multi-storied fighting castles and more tumblehome to accommodate them.
However, Henry V’s ships were sold after his death in 1422, leaving England to rely again on merchant ships for its naval defence. It was Henry VIII who founded the current Royal Navy in 1509, as a force of dedicated state-owned warships with their own dockyards and other shorebased infrastructure.

Battle of Dover (also called the Battle of Sandwich), 24 August 1217, showing the capture of the French flagship,32 Note the knarr-type hull without castles, grappling hook, axe and swords… and the men going over the side.

Battle of Sluys, 24 June 1340.33 Note the cog hulls with castles, fighting tops… and more men going over the side.
English medieval naval medicine
English medicine before 1150 had generally relied on folk traditions of leeches, charms and medicinal herbs, many being introduced by Viking, AngloSaxon and other post-Roman invaders. These traditions were gradually subsumed by clerical scribes such as Roger Bacon (c.1214 1292), a philosopher-friar whose writings advocated the study of nature through empirical observation. In referring to sources such as the Salerno medical school established after c.900 AD, these scribes led to English medicine becoming aligned with the Galenic model used by the rest of western Europe, in which the Church had become the key repository of medical knowledge. The folk-medicine herbalists and drug sellers developed into apothecaries, who became part of the Guild of Pepperers in 1180, followed by the Worshipful Company of Grocers in 1373. Although the Royal College of Physicians London was not established until 1518, the relationship between English university-educated physicians and apprenticeship-trained apothecaries had long entailed a small select group of the former catering to the nobility who could afford them, while supervising the latter selling their wares to the masses.
English medical developments during this time were also facilitated by Richard I’s Third Crusade (1189–1192), which found that many Middle Eastern powers had highly organised military medical organisations derived from the old Roman Empire, whose physicians often proved more efficient than their own. An exception was Gilbertus Anglicus, an English cleric-physician whose Compendium Medicinae (probably written between 1230 and 1250) included the first medical advice for sailors. It advised seafarers to keep clean, protect their heads from the sun, eat a moderate diet with plenty of fruit (anticipating the prevention of scurvy) and exercise. Gilbertus also anticipated a 19th century Admiralty regulation for airing clothing and bedding to rid them of fleas and lice, and even indicated that drinking water could be distilled from seawater.
The best-known medieval English cleric-surgeon was John of Arderne (1307–c.1377), who wrote over 50 manuscripts with more than 250 illustrations, the most famous being his treatise on anal fistulas. He is believed to have served as a military surgeon at the Battle of Crecy in 1346, Antwerp in 1338 and Algeciras in Spain in 1343, where gunpowder was used in battle for the first time.

Extract from John Arderne’s Fistula in Ano. The bottom-left illustration shows a probe inserted into a fistula to be met by the finger in the anus. Top left shows a ligature passed through the fistula using the probe. In the bottom right, the ligature is through all the fistulae, and the top right uses the ligatures to guide laying them open.
However, from 1139, the clergy were progressively discouraged from teaching or practising medicine outside their monasteries for financial gain.
Despite encouraging ‘houses of pity’, Pope Innocent III prohibited priests from performing surgery involving cautery or incision in 1215, while Henry III prohibited all English clergy from practising any medicine the following year.
Hence, the clergy began training the barbers who shaved their tonsures in minor procedures such as bleeding, cupping, dental extractions and lancing abscesses, which led to the founding of several barber-surgeon’s guilds throughout England, including the London Barber Surgeons Company in 1308. In 1376, the London barber-surgeons were separated from the barbers within the same company, who, despite having soon dropped the ‘barber’ prefix, did not form their own company until 1745. Meanwhile, a 1462 Royal Charter required the London Barber Surgeons Company to provide surgeons for the army and London and the navy after 1510. Hence, as many barber-surgeons would have begun their careers at the ‘houses of pity’, it would have been these young itinerants who first treated mariners ashore, which were eventually compelled or ‘impressed’ by the London Barber-Surgeons Company on behalf of the monarch to go to sea.
A Fellowship of Surgeons was founded in 1363, comprising a small pool of university-trained surgeons to serve the nobility and supervise the barber-surgeons’ guilds on similar terms as the physicians and apothecaries. Having established regulations for examining the London barbersurgeons in 1435, agreement with the company they ostensibly supervised was not reached until 1493. After a somewhat precarious existence, the Fellowship was subsumed into the latter in 1540. At that point, the new London Barber-Surgeons Company’s charter also allowed for the provision of four executed criminals per year for teaching purposes and specified that, although surgeons were not to cut hair nor barbers to perform surgery, both could continue to extract teeth.
Although an attempt was made in 1421 to combine English physicians and surgeons into one college, this failed three years later, resulting in a split within the medical profession that endured for the next 400 years. This had two crucial effects on British naval medicine: the physicians’ higher social status meant they rarely, if ever, went to sea, while ‘sea surgeons’ lacked the legal authority and expertise to treat the medical cases that came to comprise most of their workload. Putting surgeons rather than physicians on ships also reflected the assumption that they were only needed for treating battle casualties among the soldiers: sailors were not expected to be wounded because they had no direct fighting role.
As previously described, the care provided by physicians to their lord as part of their retinue meant their soldiers generally did without. It was not until 1415 that Henry V indentured his personal surgeon and physician to serve in France for 12 months during the Agincourt campaign. Although both were required to provide archers, the surgeon also had to find 12 junior colleagues who were paid the same rate as the archers hired by their master.
While their treatment of wounds caused by edged, thrown, torsion and bludgeon-type weapons would have followed the previous 1000 years of Galenic practice, the new firearms created a new type of wound characterised by greater amounts of devitalised tissue. The increased morbidity and mortality from the ensuing local and systemic infections, up to 600 years before the need to debride such wounds were recognised, led to a belief that they were poisoned by gunpowder until the French surgeon Ambroise Paré explained otherwise over a century later.
On the other hand, ‘Olroms’ included the following medical provisions for English sailors:
“If by chance any mariner be taken in sickness in the ship doing service he belongs thereto, the master ought to set him out of the ship, and seek lodging for him, and ought for to find him light, as tallow or candle, and to give him a lad of the ship for to look after him, or hire a woman to keep him, and obtain the same food as is used in the ship, that is to weight and as much as he took when he was in health, but no more, but as the master will.
And if he wants any other food, the master is not bound to get him any, but to be at his cost. And if the ship be ready to depart, it ought not to wait for him, and if he recovers, to receive his hire in paying and rebating that the master laid out for him.
And if he dies, his wife or next of kin or friend ought to have it for him.
This is the judgement.”
Although this meant English masters had to pay for lodging their sick and injured ashore, a key omission over the next 450 years was a lack of actual accommodation, despite King John allowing ‘houses of pity’ to hold fairs in exchange for admitting disabled soldiers and mariners. Furthermore, while the lack of distinction between royal and merchant ships meant these provisions applied to all sailors, those wounded in the King’s service were often treated as soldiers, whom their lord frequently abandoned on their return home. As a result, even sick or wounded seamen from the Cinque Ports could only expect temporary accommodation unless they could enter a ‘house of pity’.
This pattern of care for naval casualties began after the 1217 Dover battle. The few surviving wounded were landed at several places ashore, including the Maison Dieu Hospital, a Dover almshouse. As the number of permanently disabled mariners slowly increased, they established their own ‘masyndews’ via their craft guilds; the first at Kingston-on-Hull in 1457, followed soon after by the Cinque Ports and other south coast English harbours. However, other seamen’s guilds either relied on private citizens or contributed to other charities in exchange for access for their members. Even so, many of these ‘masyndews’ had less than 10 beds, while their standard of care varied considerably.
The Maison Dieu, Dover (now the oldest section of the Dover Town Hall), c.1830.59
Conclusion
No provision had been made for sick and injured English mariners until Eleanor recognised the need in both peace and war. Besides the absence of personalised attention for anyone other than the nobility, the slow pace of medical progress and a split medical profession, their standard care ashore reflected the contemporary ideas of Christian suffering as a part of life, which only began to change with the Church’s gradual withdrawal from being the sole repository of medical knowledge.
Despite increasing crew sizes and passenger/troop numbers throughout the medieval period, it seems likely that the voyages they undertook were too short to develop epidemic-level infectious diseases such as typhus and dysentery, or deficiency disorders such as scurvy until they began venturing beyond the Mediterranean and coastal Europe from the mid-15th century. Meanwhile, medieval English sea battles were rare and generally fought similarly to that ashore. While they typically still employed many weapons since prehistory, these had begun to be displaced by the first firearms, creating new types of wounds of greater morbidity and mortality. The first English seagoing health services were based on the assumption that it only required surgeons to treat wounded soldiers rather than sailors. Although this may have been so provided voyages were short, naval engagements few and casualties rare, the next three centuries saw more naval campaigns and expeditions fail through disease than losses in battle. Yet, Gilbertus had identified several shipboard hygiene and other preventive health measures as early as 1250, which, had they been adopted at that time, would have saved lives and made their success more likely.
Disclaimer
The views expressed in this article are the author’s and do not necessarily reflect those of the RAN or any other organisations mentioned.



