
Abstract
Purpose: This study aimed to determine if an association exists between basal levels of stress and immune mediators and military physical performance among Canadian Armed Forces members (CAF).
Methods: Blood samples from 219 CAF members (86 women and 133 men), were analysed for levels of cortisol, C-reactive protein (CRP), Adiponectin, INF-γ, TNF-α, IL-1β, IL-2, IL-6, IL-8 and IL-18. Grip strength, aerobic capacity and performance on six military physical performance tests (sandbag fortification, escape to cover, picking and digging, picket and wire carry, stretcher carry and vehicle extrication) were also assessed. A composite score for total performance was computed, based on rank scores from the six tasks.
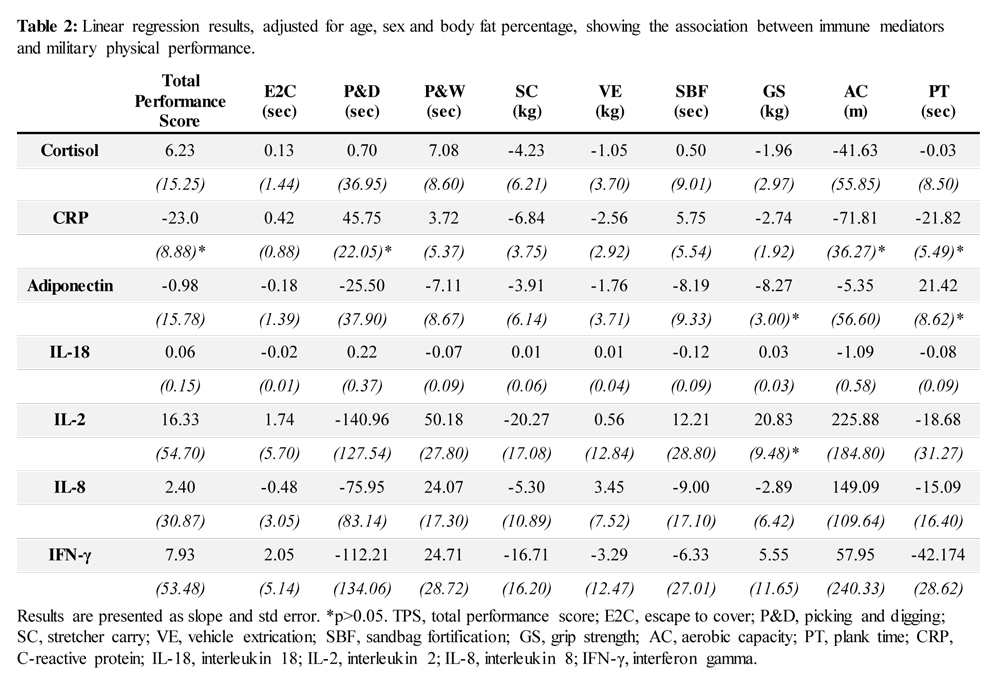
Results: The results from the linear regression analysis showed that higher CRP values were associated with lower total performance scores (slope -23.0,p≤0.05), a slower picking and digging time (slope 45.75,p≤0.05), lower aerobic capacity (slope -71.81,p≤0.05) and shorter plank time (slope -21.82,p≤0.05). A positive association between IL-2 values and grip strength was also observed (slope 20.83,p≤0.05). Adiponectin values were positively associated with plank time (slope 21.42,p≤0.05), but negatively associated with grip strength (slope -8.27,p≤0.05).
Conclusion: The results from this study suggest that high levels of immune mediators (like CRP) could be a marker of decreased military physical performance.
Key Words: inflammation, inflammatory cytokines, immune mediators, C-reactive protein, adiponectin, physical performance, Canadian Armed Forces
Introduction
Members of the armed forces are expected to maintain a high physical capacity, to be able to carry out physically demanding tasks on a frequent basis, and to meet minimum physical employment standards. Over the last decades, research has documented evidence of an association between increased levels of stress and immune mediators and a decline in physical performance. For example, elevated basal levels of C-reactive protein (CRP), IL-1β, TNF-α, and IL-6 have been linked to functional decline and a decrease in general physical performance.1-3 Brinkley et al,4 found that CRP levels were negatively associated with grip strength and performance on a Short Physical Performance Battery (balance test, timed walk, repeated chair stands) in an adult population (>55 years), and the association was age independent. Some studies have also suggested that IL-18 may be associated with a decrease in physical performance in the elderly population.5 Studies have also shown that high adiponectin levels could be negatively associated with lower physical performance and muscle strength in an
elderly population.6, 7 Toth and Matthews,8 observed a negative association between CRP levels and both
myosin heavy chain and mixed muscle protein in a large population, consisting of men and women with a wide age range, suggesting muscle protein metabolism could be part of the association linking high levels of inflammatory cytokines to a decrease in physical performance.
Members of the armed forces are at an increased risk of stress exposure.9, 10 The everyday life of a
military service member often entails stressors, such as physical and environmental stress stemming from occupational tasks, concern about potential relocation, deployment in combat operations and the strive for promotion.11 Studies by Pflanz and Sonnek,11 and Pflanz et al,12 showed that as many as 26% of US Air Force service men and women reported to suffer from work related stress. 15% reported that work stress was causing them significant emotional stress. High stress levels have been linked to an increase in the production of inflammatory cytokines.13, 14 Previously published results from our group have also shown that CRP levels in the Canadian Armed Forces (CAF) increase with age, and we also observed an increase of inflammatory cytokines with age.15 CAF members are required to possess a minimum physical capacity to carry out occupational tasks and meet minimum physical employment standards; however, no previous study has investigated the association between basal levels of immune mediators and physical performance on a discrete test battery among members of the armed forces. Therefore, the purpose of this study was to determine if an association exists between basal levels of cortisol, adiponectin and inflammatory cytokines, and performance on a discrete battery of military physical performance tests in a representative sample of the CAF. Based on previous findings, it was hypothesised that levels of stress and immune mediators would be negatively associated with military physical performance.
Methodology
Participants
In order to assess the association between levels of cortisol and cytokines and military physical performance in a military population, blood draws were collected from a representative sample of regular force CAF members (n=219). All blood samples and measurements were collected as a part of the development of a new physical employment standard for the CAF. All participants were prescreened prior to taking part in the study, where resting blood pressure and heart rate were recorded, and participants completed the Physical Activity Readiness Questionnaire (ACSM, 16) and the Risk Stratification Questionnaire (ACSM, 17). Participants having any medical conditions or restrictions limiting their ability to perform physical tasks were excluded from the study. Also, participants identified as ‘high risk’ according to the Risk Stratification Questionnaire (symptomatic or known cardiovascular, pulmonary or metabolic disease). Pregnant women were also excluded from participating in the study. The study was conducted following the guidelines of the Helsinki Declaration and received ethics approval from Defence Research and Development Canada’s Human Research Ethics Board and The University of Ottawa Research Ethics Board.
Anthropometric data
Height was measured using a Seca 213 Portable stadiometer (Seca Industries, Hanover, Maryland, USA). Hip and waist circumference were measured using a standard measuring tape. Waist circumference was measured at the superior edge of the iliac crest, and hip circumference was measured at the widest part of the buttocks. Body weight
was measured using a standardised and calibrated professional grade digital weighing scale (Health-ometer, Alsip, Illinois, USA). Body composition was estimated through bioelectrical impedance analysis, using the InBody 520 (BioSpace Technologies, Los Angeles, USA), previously validated against Dual Energy X-ray Absorptiometry.
18 Body composition was estimated in the morning, and participants were asked to refrain for exercise prior to arrival, and to arrive well hydrated. The body composition analysis gave an estimate of lean body mass (LBM) and fat mass and, based on these estimates, body fat percentage (BF%) was calculated. BMI was calculated by dividing body weight by height squared (weight (kg)/height2 (m)).
Blood sample collection
Participants were instructed to be fasted, avoid consuming caffeinated beverages and nicotine during the 2 hours prior to testing, and not to exercise or consume alcoholic beverages for 6 hours prior to testing. Blood samples were collected in the morning, upon arrival in the laboratory, by a qualified laboratory technician. All blood samples were collected before any exercise testing was performed. Blood samples were collected in 6 mL EDTA tubes
and immediately placed on ice until centrifugation at 2428 x g. Plasma was separated in 2 mL aliquots and stored in a -80oC freezer until analysis.
Blood sample analysis
All blood samples were analysed for levels of cortisol, adiponectin, CRP, INF-γ, TNF-α, IL-1β, IL-2, IL-6, IL-8 and IL-18. These markers were selected based on having a high detection rate in this specific population, and previous studies showing these specific markers to be associated with physical performance in the general population.1, 2, 5, 7 Cortisol was measured using a Parameter Cortisol Assay (R&D Systems, Minneapolis, MN, USA), while CRP and adiponectin were measured using a Human C-Reactive Protein ELISA and the Human Adiponectin Platinum Sandwich ELISA kit (Affymetrix eBiosciences, San Diego CA USA). All assays were performed as instructed by the manufacturer. Each plate had a standard curve in duplicate and all plates were read at 450 nm in the Elisa plate reader FilterMax F5 Multimode microplate reader (Molecular Devices, Sunnyvale CA). The SoftMax Pro 6.2.2 (Molecular Devices, Sunnyvale CA) software was used to determine the levels of cytokine in the unknown, using the standard curve found on each plate. The levels of IFN-γ, TNF-α, IL-1β, IL-2, IL-6, IL-8 and IL-18 were determined using the Procarta Plex Multiplex Immunoassay (Affymetrix eBiosciences, San Diego CA USA). Samples were prepared and used as instructed by the manufacturer of the kits. Standard curves were run on each plate together with unknowns. The plates were read on the luminex MAGPIX instrument (Affymetrix eBiosciences, San Diego CA USA) and the cytokine levels for each unknown were extrapolated from the standard curves using the Procarta Plex analyst software with either a 4 or 5 parameter logistic curve of the standards. The same procedures and assays used to determine cortisol and cytokine levels in plasma have been used in previous publications,19, 20 and the coefficients of variation of the standards were 5.6% (IFN- γ), 4.5% (TNF-α), 3.1% (IL-1β), 3.6% (IL2), 9.8% (IL-6), 4.5% (IL-8), 5.6% (IL-18), 13.8% (adiponectin), 13.2% (CRP) and 11.6% (cortisol).
Physical capacity and military physical performance measures
Military physical performance was measured on six military specific tasks. These tasks were sandbag fortification (lifting and moving sandbags), escape to cover (obstacle course resembling an escape to cover under fire task), picking and digging (separate picking and digging simulators), pickets and wire carry (resembling carrying equipment for a fence erection) and stretcher carry and vehicle extrication (resembling extracting a wounded service member from a disabled car). A more detailed description of each task can be found in Tingelstad et al.21
Performance on the sandbag fortification, escape to cover, picking and digging, and pickets and wire carry task was measured as time to complete the task. For the stretcher carry and vehicle extrication task performance was measured as maximal load lifted and carried. Total performance was calculated by ranking each individual score and giving it a percentile score (best performance = 100, lowest performance = 1) based on rank order. To estimate aerobic capacity, a multistage 20-meter shuttle run test was used. This test has previously been validated and found to accurately represent a measure of aerobic capacity,22 and the procedures for the tests are described in the CF EXPRES Operations Manual.23 The level attained and the number of stages completed on that level was recorded and converted into total distance covered (m). Grip strength was used as a measure of upper body strength. Grip strength has been found to be a valid predictor of total upper body strength in young adults24 and was measured using a Smedly Analog hand dynamometer (Smedly TTM, Tokyo, Japan). The procedures for grip strength measurement can be found in the CF EXPRES Operations Manual.23 Following standard protocol, grip strength was measured twice for both left and right hand, and the highest recorded measurement for each hand was summed and used as the measure of grip strength.
Abdominal muscular endurance was measured using a maximal prone plank time (seconds) protocol. Having forearms and toes place on the ground, participants were asked to lift their hips of the ground and maintain a neutral spine. The test was terminated when the participant failed to maintain a neutral spine. Detailed descriptions of
procedures are found elsewhere.25 Each participant’s physical performance measures and blood sample were collected on the same day.
Statistical analysis
Due to non-normal distribution, all cytokine values were log10 transformed before any statistical analyses were performed. As men and women are held to the same physical employment standard and performed the same physical performance test, male and female data were combined into one cohort. Multiple linear regression analysis was used to determine the association of cytokine levels on military physical performance. With age, sex and BF% being covariates of both cytokine levels and performance,26-30 the regression model was adjusted
for these factors. Results from the linear regression analysis were presented as slope and standard error.
Significance level was set to p≤0.05. All statistical analyses were performed using SPSS 23.0 (IBM SPSS Statistics for Windows, Version 23.0, IBM Corp, Armonk, NY).
Results
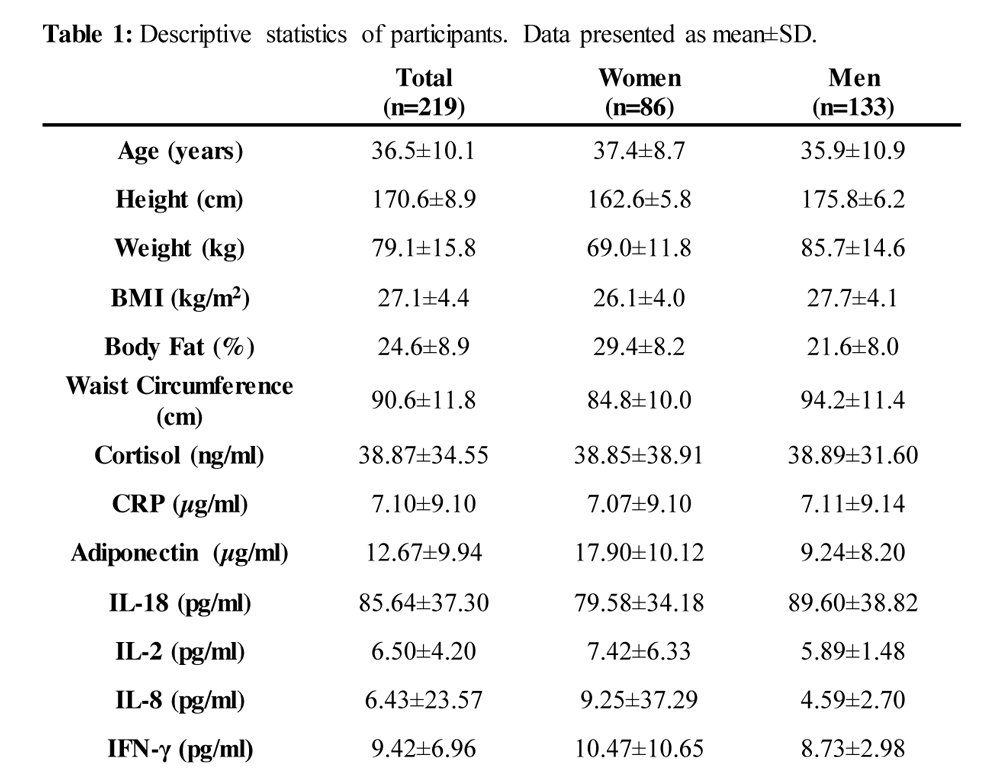
Performance data and blood samples from a total of 219 CAF members were made available for this analysis. A detailed description of participant characteristics can be found in Table 1. The results from the blood sample analysis showed a low detection rate of IL-1β, IL-6 and TNF-α. Only 4%, 4% and 2% of men, and 5%, 6% and 3% of women had measureable values of IL-6, TNF-α and IL-1β respectively. Due to the low rate of measureable values, these inflammatory cytokines where excluded from further analysis.
Results from the multiple linear regression analyses are found in Table 2. There were no observed associations between cortisol, IL-18, IL-8, IFN-γ or any of the physical performance measures recorded. Higher CRP levels were associated with a decrease in military physical performance. A negative association was observed between CRP levels and: aerobic capacity (p≤0.05), plank time (p≤0.05), picking and digging performance (p≤0.05) and total performance (p≤0.05). A negative association between adiponectin levels and grip strength (p≤0.05), was observed; however, higher adiponectin levels were also associated with an increase in plank time (p≤0.05). Interleukin 2 was found to be positively associated with grip strength (p≤0.05), where higher IL-2 levels indicated better grip strength. No other association between cytokine levels and physical performance were observed.
Discussion
Members of the CAF are required to possess a minimum physical capacity to perform occupational duties; however, the high stress exposure associated with being a member of the armed forces could potentially have a negative impact on military physical performance. This study is the first to investigate if an association exists between basal levels of cortisol, adiponectin and inflammatory cytokines and performance on a discrete physical performance battery in the CAF. Results showed a negative association between CRP levels and military physical performance, where high levels of CRP were associated with a decline in total performance, picking and digging time, plank time and aerobic capacity. Higher adiponectin levels were associated with lower grip strength, but improved performance on the front plank task. Based on these results, there seems to be an association between levels of inflammatory cytokines and military physical performance, which could potentially mean that individuals with high levels of stress and immune mediators might be at a disadvantage when it comes to performing military tasks and physical performance tests.
C-reactive protein and military physical performance
C-reactive protein is an acute phase protein, produced by the liver during the initial stage of an inflammatory reaction, and is a potent marker for the presence of an inflammatory reaction.31, 32 Previous studies in the elderly population have suggested a negative association between CRP levels and physical performance. Similar results were observed in CAF members. The results from the multiple linear regression analyses showed a negative association between CRP levels and aerobic capacity, plank time, picking and digging performance and total performance (Table 2). Few studies have assessed the association between inflammatory cytokines and physical performance in a military population, but studies from the general population have found similar results. Taaffe et al,1 found that higher CRP levels were associated with poorer grip strength. They also observed a trend towards lower CRP levels in people with faster walking speeds. A cross-sectional study conducted by Norman et al,33 showed an independent inverse relationship between CRP levels and handgrip strength. The inverse association between CRP and grip strength did not reach significance in our cohort (p=0.156). However, CRP levels were found to be inversely related to performance on the picking and digging task, plank time and aerobic capacity. The results from this study seem to indicate a negative association between CRP levels, independent of age, sex and adiposity and military physical performance.
Adiponectin and military physical performance
The adipokine adiponectin plays a crucial role in glucose regulation and lipid metabolism,34 and is considered to have anti-inflammatory effects.35 High plasma concentrations of adiponectin have also been associated with a lower BMI and lower waist circumference.36, 37 Based on the association between high levels of adiponectin and lower BMI and waist circumference, we expected, if any, a positive effect of adiponectin on physical performance in this military population. Instead, an inverse relationship between adiponectin levels and grip strength was observed (Table 2) suggesting high adiponectin levels to be negatively associated with physical performance. Previous research has found similar results in studies in an elderly population, where a significant inverse relationship between physical performance, muscle strength and adiponectin levels have been shown.6, 7 It is therefore likely that the negative relationship between adiponectin and physical performance could be explained by an inverse relationship between adiponectin levels and body mass, and more specifically LBM,36 rather than a direct negative effect of adiponectin on physical performance. As previously described, adiponectin levels increase with a decrease in BMI and body mass. This has been associated with a decrease in LBM in the elderly population.6, 7 Unpublished data from our lab showed a negative correlation between adiponectin levels and LBM in a military population, which could explain the inverse relationship found between adiponectin levels and grip strength in this study (the current study was a part of a large research project, and the LBM data points will be published in a future publication). Participants with higher adiponectin levels also recorded a better plank time, compared to participants with lower adiponectin levels. This could also be explained by an inverse relationship between adiponectin levels and body mass. Previous studies have shown a negative correlation between plank times and body mass, where people with a higher body mass (i.e. lower adiponectin levels) had a lower plank time.38 Based on these results, it seems that rather than having a direct effect on physical performance, changes in adiponectin level could serve as a marker of change in body composition, which could again affect physical performance.
The results from this study are not able to determine the specific cause of the association between inflammatory cytokines and military physical performance. If one were to speculate, it is known that mental and physical stress exposure itself can affect physical performance,39 and clear evidence exists of a connection between stress level, immune system activation and release of inflammatory cytokines.13, 14 It is also known that inflammation and proinflammatory cytokines play a role in muscle wasting, and high levels of cytokines like TNF-α and IL-1β measured in muscle tissue, have been associated with muscle wasting and a decrease in muscle mass.40 It is therefore possible that high levels of pro-inflammatory cytokines in circulating plasma could be a marker of an ongoing inflammatory reaction in the muscle, rather than high levels of cytokines in circulating plasma having a direct negative effect on physical performance. These are only speculations of potential pathways linking inflammatory cytokines and physical performance, and more research is required to clarify the cause and effect of inflammatory cytokines on physical performance. However, based on these results, strategies to decrease inflammation and levels of inflammatory cytokines, could be beneficial to improve military physical performance. Several anti-inflammatory drugs are available (e.g. corticosteroids, Aspirin), which have been found to decrease levels of pro-inflammatory cytokines.41 Regular physical exercise42 and sufficient sleep43 have also been shown to be beneficial to decrease levels of pro-inflammatory cytokines. This study was not designed to answer such questions; however, potential anti-inflammatory strategies and their effect on military physical performance should be elucidated in future studies.
Limitations
The models used in this study to determine the association between cortisol and cytokine levels and military physical performance were adjusted for age, sex and adiposity, which are all known to affect cortisol and cytokine levels. Other factors, such as fasting status,44 ethnicity45 and medication (e.g. aspirin),46 can also affect cortisol and cytokine levels, but due to this being a secondary analysis of previously collected data, we were unable to control for these variables.
There are also several factors affecting the rate of transcription, translation and breakdown of cytokines (e.g. exercise,47 acute stress exposure,13 as well as their circadian fluctuation48 and differences in half-life. CRP’s half-life is ~19 hours,49 whereas IFN-gamma has a half-life of only a few minutes.50 Certain cell types contain cytokines prepackaged in vesicles, which can be released immediately upon stimulation.51 Therefore, cytokine levels measured in blood samples collected in the morning might not be a perfect representation of plasma values later in the day. There are also known limitations to bioelectrical impedance analysis, used to determine body composition. Obesity level, body geometry, total body water and body water distribution are all factors known to influence the results of bioelectrical impedance analysis.52 However, this participants sample did not have a high level of obesity or BMI (Table 1), and were encouraged to drink water prior to and throughout the data collection day, so the impact of these factors on body composition should be minimal. To follow up on this, a controlled study should be performed comparing physical
performance between people with normal and high basal cytokine levels, as well as collecting blood samples pre- and post-exercise. Research has shown that regular evaluation of hormone levels can be a tool used in preventative and personalised medicine,53, 54 and future studies should investigate the potential of using regular evaluation of stress and immune mediators as a tool to predict changes in military physical performance.
Conclusion
This study is the first to assess the association between basal levels of cortisol, inflammatory cytokines and performance on a discrete physical performance battery in a military population. There was no observed association between cortisol, IL-18, IL-8, IFN-γ and any of the outcomes of the military physical performance test. However, CRP levels were negatively associated with total military physical performance, aerobic capacity, plank time, picking and digging performance and adiponectin levels were negatively associated with grip strength, confirming
the hypothesis. On the other hand, adiponectin levels were also positively associated with plank time, and IL-2 was positively associated with grip strength. Even though more research is needed to confirm these results, the results of this study seem to indicate an association between CRP levels and military physical performance. The potential negative effect of pro-inflammatory cytokines on military physical performance could be a part of the explanation of why certain CAF members might struggle to meet the physical employment standard. Based on these results, developing strategies to decrease inflammation in CAF members with high levels of pro-inflammatory cytokines, could help to improve military physical performance.
Corresponding author: Hans Christian Tingestad, hans.chr.tingelstad@gmail.com
Authors: H Tingelstad1, L G Filion2, J Martin1,4, M Spivock1,3, V Tang3, F Haman1
Author Affiliations:
- School of Human Kinetics, Faculty of Health Sciences, University of Ottawa, Ottawa, Ontario, Canada/li>
- Department of Biochemistry Microbiology and Immunology, Faculty of Medicine, University of Ottawa, Ottawa, Ontario Canada/li>
- Canadian Forces Morale and Welfare Services, Directorate of Fitness, Ottawa, Ontario, Canada/li>
- University of Ottawa Flow Cytometry Core Facility, Ottawa, Ontario, Canada



