
Abstract
Irritable bowel syndrome (IBS) is a disorder of gut-brain interaction (DGBI) that affects about 10% of the adult population in the United States. IBS pathoetiology understanding has evolved and clinical management improved despite the underdevelopment of diagnostics. Within the Veterans Affairs (VA) system, the prevalence and impact of DGBIs are high. Yet there is a paucity of information on the patient demographic features. Our team examined the history and workup of patients referred to an IBS clinic within the VA’s gastroenterology service through a systematic case series study to begin a quality improvement initiative.
Introduction
Despite its prevalence, irritable bowel syndrome (IBS) remains a poorly understood disorder of gut-brain interaction (DGBI) or functional gastrointestinal disorder (FGID).1,2 A recent population-based study focusing on Gulf War era veterans found that IBS was the fifth most common health condition among deployed female (30.2%) and male veterans (23.9%).3 Veterans are unique because they encounter deployment exposures (enteric infections, occupational/environmental contacts) and often have mental health comorbidities underlying their disease. However, very little has been described regarding patient demographic features, presentation and diagnostic strategy. Therefore, as part of a quality improvement initiative to inform improvements in primary care-based management, an initial case series study was conducted to understand the characteristics, illness history and initial evaluation of patients referred to a new IBS clinic in the gastroenterology service of our VA medical centre.
Methods
Patients with possible prior IBS diagnoses were referred to the IBS clinic by VA gastroenterologists and primary care clinicians. A standardised data extraction form was developed and used to extract de-identified patient data from the following sources. Information on demographics, prior history, service experience, disability, medications and medical comorbidities were retrieved from the Computerized Patient Record System and Joint Longitudinal Viewer electronic health records (EHRs). Further information included Rome Criteria,4 Bristol Stool Scale type,5 IBS symptom severity scores (IBS-SSS),6 Hospital Anxiety and Depression scores (HADS),7 General Practice Physical Activity Questionnaire categorisation,8 most bothersome symptom(s) and treatment history. The EHR was comprehensively reviewed to accurately determine the dates of gastrointestinal (GI) symptom onset, first chronic bowel dysfunction diagnosis (if applicable) and IBS diagnosis (if applicable). Data were entered into Microsoft Excel (Redmond, WA) and descriptively analysed by Stata IC/SE Version 16 (College Station, TX).
Results
Over eight months, 11 consecutively referred patients were included in the case series with a median age of 43 years, all male, majority Caucasian (81.8%) and predominantly from the Persian Gulf War (72.7%), post-Vietnam (18.2%) and Vietnam (9.1%) eras (Table 1). A median of 4 (interquartile range [IQR] 2.5–14.5) years from self-reported symptom onset to the first diagnosis of chronic bowel dysfunction diagnosis was observed (Table 2). The first diagnosis recorded in the patient’s EHR was most often IBS (66%), followed by functional and chronic diarrhoea. Utilising Rome Criteria by excluding alternative aetiologies, a median of 9 (IQR 3–15) years between first symptom onset and confirmed IBS diagnosis was recorded. Two patients did not have IBS but rather an organic disease discovered during workup in the IBS clinic. Median IBS-SSS was 270 (IQR 206–367), with 40% of patients meeting the criteria for severe IBS. Our population’s Bristol Stool Scale distribution is skewed rightward, indicating a looser stool type predominance (Figure 1). Co-morbid anxiety and depression were common, with 30% and 40% identified on the HADS, respectively. The majority of patients were physically inactive. Many had mental health diagnoses, and some were noted to be taking daily medications with off-target GI side effects, including selective serotonin reuptake inhibitors (1/11), calcium channel blockers (3/11), alpha receptor blockers (2/11) and serotonin/norepinephrine reuptake inhibitors (1/11). Cramps, diarrhoea, gas, bloating and urgency were the most frequently reported bothersome symptom. Red flag symptoms were present in several patients. When evaluating the current practice in diagnostic workup among patients referred to the IBS clinic, the minority of patients met the current standards of a positive diagnostic workup (Table 3).
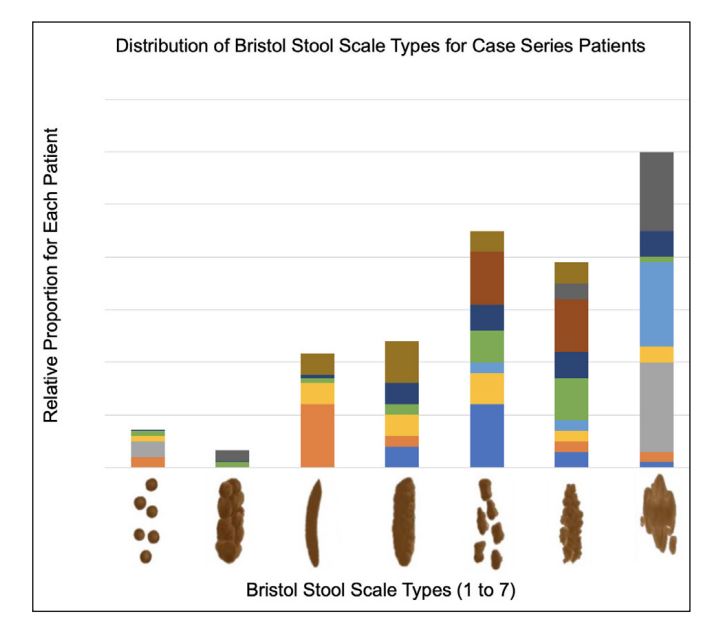
Figure 1. Each colour represents one individual patient and the relative proportion of bowel movements they passed at each stool consistency during the average week.
Table 1. Demographic characteristics of veterans who were referred to IBS clinic
| Parameter | Median (IQRa) or n/N (%) |
|---|---|
| Age, years | 43 (39–48) |
| Male sex | 11/11 |
| Race/Ethnicity | |
| White | 9/11 (81.8%) |
| Asian | 1/11 (9.1%) |
| Unspecified | 1/11 (9.1%) |
| Hispanic/Latino | 0/11 |
| Branch of Service | |
| Navy | 5/11 (45.5%) |
| Army | 4/11 (36.4%) |
| Marine Corps | 2/11 (18.2%) |
| Period of Service | |
| Persian Gulf War | 8/11 (72.7%) |
| Post-Vietnam | 2/11 (18.2%) |
| Vietnam Era | 1/11 (9.1%) |
| Service connection, % disabled (n=10) | 90 (57.5–100) |
| Number of comorbid conditions | 10 (6–15) |
| Number of oral medications | 9 (5–10) |
Table 2. Clinical presentation of veterans during initial visit to IBS clinic
| Parameter | Median (IQRa )or n/N b(%) |
|---|---|
| Years from symptom onset to first functional gastrointestinal disorder diagnosis (n=9) |
4 (2.5–14.5) |
| First functional gastrointestinal disorder diagnosis (n=9) | |
| IBS-D | 3/9 (33.3%) |
| IBS-M | 2/9 (22.2%) |
| IBS-U | 1/9 (11.1%) |
| Functional diarrhoea | 2/9 (22.2%) |
| Chronic diarrhoea | 1/9 (11.1%) |
| Years from symptom onset to IBS diagnosis (n=7) | 9 (3–15) |
| IBS phenotype (n=7) | |
| IBS-D | 4/7 (57.1%) |
| IBS-M | 2/7 (28.6%) |
| IBS-U | 1/7 (14.3%) |
| IBS-Symptom Severity Score (n=10), 0–500 | 270 (206–367) |
| Moderate (175–300) | 6/10 |
| Severe (300–500) | 4/10 |
| Hospital Anxiety and Depression Scale-Anxiety (n=10), 0–21 | 9.5 (6.8–16.8) |
| Normal (0–7) | 3/10 |
| Borderline abnormal (8–10) | 4/10 |
| Abnormal (11–21) | 3/10 |
| Hospital Anxiety and Depression Scale-Depression (n=10), 0–21 | 4 (1.8–4.5) |
| Normal (0–7) | 6/10 |
| Borderline abnormal (8–10) | 0/10 |
| Abnormal (11–21) | 4/10 |
| General Practice Physical Activity Questionnaire (n=10) | |
| Active | 3/10 |
| Inactive | 7/10 |
| Most bothersome symptom(s) (n=10) | |
| Diarrhoea | 4/10 |
| Constipation | 1/10 |
| Cramps | 6/10 |
| Gas/bloating | 3/10 |
| Urgency | 3/10 |
| Frequency | 2/10 |
| Incontinence | 1/10 |
| Perceived incomplete evacuation | 1/10 |
| Haemorrhoids/rectal bleeding | 2/10 |
| Borborygmi | 1/10 |
| Red flag symptoms (n=10)c | |
| Nocturnal symptoms | 4/10 |
| Blood in stoold | 3/10 |
| Unintentional weight loss | 1/10 |
a IQR = interquartile range
b One patient excluded due to incomplete IBS clinic intake
b No patients with fever or iron deficiency anaemia, or family history of IBD, CRC or CeD
c Does not distinguish haemorrhoids/fissures
Table 3. Adherence to IBS diagnostic guidelines in veterans referred for care at IBS clinic
| Guideline Standard | n/N a |
|---|---|
| Completed coeliac disease testing | 4/10 |
| Completed fecal calprotectin or lactoferrin testing | 3/10 |
| Completed c-reactive protein testing | 4/10 |
| Avoided fecal ova or parasite testing | 8/10 |
| Completed colonoscopy if red flags and/or over 50 years b | 9/10 |
| Completed colonoscopy if no red flags and/or under 50 years | 1/10 |
b Data was collected before updated CRC screening guidelines changed to 45 years
Discussion
Diagnosis and management are essential when optimising outcomes and improving the quality of life in persons with medically unexplained illnesses, including DGBI.9 Several important observations were made from this case series. First, there was a noteworthy delay from time of
symptom onset to the first EHR-documented chronic DGBI/FGID diagnosis. Diagnostic delay occurs in many populations with GI conditions. It is known to greatly increase the burden of disease and healthcare utilisation.10 Second, among our cohort of Veterans, there was a high level of mental health comorbidities (8 of 11 had at least one mental health diagnosis), as well as the use of medications with known GI side effects. While the genesis of GI symptoms often predated the start of these medications, it may be important to consider working with mental health professionals to optimise treatment regimens for both GI and mental health conditions. A future study may be indicated to explore medication interactions and disease management in Veterans with mental health disorders and DGBI. Finally, these data provide an initial assessment of the current practice patterns of diagnostic workup of patients with chronic GI complaints. Within the group of patients referred to the IBS clinic, we observed that a positive diagnostic strategy with the utilisation of Rome Criteria-based definitions for IBS, plus a limited amount of stool testing and referral for colonoscopy was not universally performed, despite existing contemporary expert reviews and guidelines. These guidelines suggest that IBS should not be made as a diagnosis of exclusion but rather a confident, positive diagnosis after other conditions (inflammatory bowel disease, coeliac disease, enteric infection) have been ruled out.11 Of the referred patients with possible IBS, two ultimately did not (one had coeliac disease, and one had severe disaccharidase deficiency with malabsorption). These observations will form the basis of future studies and initiatives to optimise the diagnosis and management of veterans with IBS by improving provider awareness of current clinical guidelines. While these findings are valuable, they are also limited and require caveats. The sample population was not a random sample of veterans with IBS. It likely reflected the selection of more severe cases referred from providers in the gastroenterology service or primary care providers with challenging patients. Future systematic investigations of veterans with IBS diagnoses not seen by gastroenterologists are needed to more appropriately describe the patient population and their management. Furthermore, the results from this study reflect the experience of one VA medical centre and are unlikely to be generalisable to patient experiences at other centres.
In summary, we believe these data support the need to investigate DGBI further among veterans to advance the development and utilisation of effective diagnostic and treatment techniques directed towards the underlying pathogenesis and holistically consider the contributions of both the psychological and GI facets of the condition. For IBS and other medically unexplained illnesses common in veteran populations, we know that building a trusting and quality relationship between patient and provider is critical for improving health outcomes and quality of life.12 Advancing provider education through quality improvement initiatives that emphasise the utilisation of positive diagnostic strategies, evidence-based treatments and the formation of a healthy provider-patient relationship are attainable goals that will likely improve the quality of care for veterans with IBS.
Corresponding Author: Pierce Landon Claassen, pierce.claassen@wsu.edu
Authors: P L Claassen1, T Hinojosa2, A Rai2, M S Riddle2
Author Affiliations:
1 Washington State University Elson S Floyd College of Medicine
2 VA Sierra Nevada Health Care System