
Introduction
Musculoskeletal injuries are a common occurrence during the period of basic military training (BMT). During the BMT period, it is estimated that 25% of male and 50% of female trainees experience injuries. In a review of Army basic training, injury risk-factor studies showed that increased age, smoking history and prior sedentary lifestyle among male recruits were associated with increased injury risk.
Low physical conditioning is strongly associated with an increased risk of training-related musculoskeletal injuries in military trainees. In particular, poor performance on timed run tests with a fixed distance is a predictor for injuries. In a study performed in the British Army, 58% of 1810 recruits sustained at least one injury during initial military training. Overuse musculoskeletal injuries were more common than acute injuries, representing 65% and 35% of injuries, respectively.
Studies for musculoskeletal injuries among Greek Army Officer cadets during combat BMT revealed that 32% presented with injuries (muscle, tendon, bone, joint and ligament)8 and 28.3% suffered from some form of injury, with 51.3% appearing during the first two weeks of BMT.
The purpose of the present study was to focus on the effects of military combat uniforms compared to athletic clothing on injury rates during BMT in Greek naval cadets.
Methods
Subjects
Forty-five healthy male Greek Naval cadets volunteered to participate in this study. Their mean values ± standard deviation (SD) was for age 18.2 ± 0.5 years, body mass 75.9 ± 3.8 kg and body height 177.7 ± 4.6 cm. The cadets were randomly separated into two groups, both of which exercised with the same training protocol but different clothing. Group1, which included athletic clothing (AT), exercised with sports shorts, a t-shirt and sports shoes (n=21, age 18.2 ± 0.5 years, body mass 76.1 ± 3.8 kg and body height 178.6 ± 5.7 cm). Group2 trained with military clothing (MT) and boots (n= 24, age 18.3 ± 0.6 years, body mass 75.6 ± 3.3 kg, and body height 176.8 ± 2.3 cm) as shown in Table 1.
The study’s results involved only the Naval cadets who completed BMT and who abstained from exercise owing to injuries for up to three days. All the Greek Naval cadets were healthy, non-smokers and had no injuries the two years prior to the BMT.
Table 1. Anthropometric measurements and body composition
| Group | AT (n=21) | MT (n=24) | Total (n=45) |
|---|---|---|---|
| Age (years) | 18.2 ± 0.5 | 18.3 ± 0.6 | 18.2 ± 0.5 |
| Height (cm) | 178.6 ± 5.7 | 176.8 ± 2.3 | 177.9 ± 4.6 |
| BM (kg) | 76.1 ± 3.8 | 75.6 ± 3.3 | 75.9 ± 3.8 |
| BMI (kg×m2) | 23.9 ± 1.6 | 24.2 ± 1.1 | 24.0 ± 1.4 |
| BF (%) | 11.2 ± 3.8 | 10.5 ± 2.8 | 11.1 ± 3.4 |
BM = Body Mass; BMI = Body Mass Index; %BF = percentage of Body Fat; cm = centimetres; kg = kilogram
Training protocol
The BMT period lasted five weeks. The training program was applied six times a week from Monday to Saturday, four days included physical fitness and two swim training sessions. In the first week, three days were used for the following measurements: anthropometric (height, body mass, body mass index calculated as weight in kilograms divided by height in metres squared and % fat) and physical fitness tests (push-ups in one minute, sit-ups in one minute and 12 minutes run test).
The Naval cadets that participated in the BMT performed 27 training sessions in the morning and 27 in the afternoon. The morning training sessions lasted 70 minutes and included 3 x 12 min running with a five min interval, followed by 24 minutes of agility exercises, gymnastics, sit-ups, pushups, rope climbing, obstacle course training and stretching. The swimming training sessions lasted 50 mins. The groups ran at a standard pace of 6:30 min/km for weeks 1–2, 6:00 min/km for weeks 3–4 and 5:30min/km for week 5 (Table 2).
Furthermore, in the afternoon from 17:00–18:00, all cadets participated in marching-military activity sessions for 60 minutes.
Statistical analysis
Data are presented as mean (± SD). A two-proportion z-test was used to test for the statistically significant difference between the two population proportions on injuries. Significance was accepted at P < 0.05.
An injury was registered when cadets felt pain or complained of pain during BMT and visited a military physician. Musculoskeletal injuries recorded were muscle pain, tendon, stress fracture and joint or ligament injury (knee pain, ankle pain). Additionally, every injury requiring a cadet to consult a physician (unit medical officers and conscripted physicians) was registered and documented.
Results
The data was recorded for 22 Naval cadets from the MT group, because two cadets dropped out in week 2 of the BMT. From the results, there was a significant difference in the proportion of injuries between the two groups (z = -2.3044, P = 0.021, P < 0.05). The injuries occurred in six (28.6%) Naval cadets from the AT group and 14 (63.6%) Naval cadets from the MT group, totalling 20 injured cadets. During the five weeks of BMT, 36 injuries were recorded, for AT six (16.7%) injuries and MT 30 (83.3%) injuries. Both groups recorded 18 (50.0%) joint/ligament injuries, six (16.7%) stress fractures, eight (22.2%) tendon and four (11.1%) muscle injuries. Specifically, the AT group recorded six injuries, of which four (66.6%) were joint/ligament injuries, one (16.7%) a stress fracture and one (16.7%) a tendon injury. In addition, the MT group recorded 14 (46.7%) joint/ ligament injuries, five (16.7%) stress fractures, seven (23.3%) tendon and four (13.3%) muscle injuries. The injury ratio (injuries per trainee) was 0.3 injuries per trainee in the AT team and 1.4 injuries per trainee in the MT team (Table 3). The incidence of injuries in each week of BMT was seven in week 1, 12 in week 2, 13 in week 3, four in week 4 and none in week 5 (Table 4, Figure 1).
| Exercises per week | ||||||
| week | Monday | Tuesday | Wednesday | Thursday | Friday | Saturday |
| 1 | Test day 1 | Test day 2 | Test day 3 | Physical fitness | Physical fitness | Swimming |
| 2-5 | Physical fitness | Physical fitness | Swimming | Physical fitness | Physical fitness | Swimming |
| Training sessions | ||||||
| Exercise | Total | |||||
| Morning 6:00–7:10 | (3×12 min running /5 min interval /common pace 6:30 min/km for weeks 1–2, 6:00 min/km for weeks 3–4 and 5:30min/km week 5) + (24 minutes exercises/ agility, gymnastics, sit ups, push-ups, rope climbing & stretching) Swimming training sessions lasted 50 min |
27 | ||||
| Afternoon 17:00–18:00 | 60 min/marching-military activity | 27 | ||||
Discussion
This study aimed to investigate the effects of training with sports clothing and military combat uniform and boots on the occurrence of injuries during five weeks of BMT. The training with military combat uniform and boots caused injuries to 20 Naval cadets, corresponding to 46.5% of those who completed the BMT. In the AT group, six cadets (28.6%) were recorded with injuries, and in the MT group 14 cadets (63.6%) recorded injuries. Research in BMT in the Greek Army cadets reported injuries in 32.0%8 and 28.3%9 of the trainees, which is a close percentage compared to the AT team, which presented 28.6%. However, in the MT group’s current recording, 63.3% of injured cadets is double that of the above studies in the Greek Army.
The results showed that during the BMT period, both groups showed a total of 36 injuries, of which 30 (83.3%) occurred in the MT group and six (16.7%) occurred in the AT group. Fifty per cent of the injuries in both groups occurred in the joints and ligaments, four of which were in the AT group and constituted 66.6% and 14 in the MT group 46.7%, respectively. The other injuries presented in the AT group were one stress fracture and one tendon corresponding to 16.7% each with no muscle injury. Respectively, in the MT group, there were five cases of stress fracture (16.7%), seven cases of tendon injury (23.3%) and four of muscle injury (13.3%). The injury ratio was 0.3 injuries per trainee in the AT team and 1.4 injuries per trainee in the MT team. Injuries reported during BMT are consistent with research on the BMT period and report the occurrence of injuries.
Table 3. Results
| Group | AT (n=21) | MT (n=22) | Total (n=43) |
|---|---|---|---|
| Injured cadets/group | |||
| 6 (28.6%) | 14 (63.7%) | ||
| Injuries/group | |||
| 6 (16.7%) | 30 (83.3%) | 36 (100.0%) | |
| % Injuries | |||
| joint/ligament | 4 (66.6%) | 14 (46.7%) | 18 (50.0%) |
| stress fracture | 1 (16.7%) | 5 (16.7%) | 6 (16.7%) |
| tendon | 1 (16.7%) | 7 (23.3%) | 8 (22.2%) |
| muscle | 0 (00.0%) | 4 (13.3%) | 4 (11.1%) |
| Total | 6 (100.0%) | 30 (100.0%) | 36 (100.0%) |
| Injured cadets | |||
| 6 (30.0%) | 14 (70.0%) | 20 (100.0%) | |
| Injury ratio | |||
| Total | 0.3 | 1.4 | |
Injure ratio = number of injuries per trainee; % injuries = percentage of injuries
Table 4. Injuries per week
| Injuries | Week 1 | Week 2 | Week 3 | Week 4 | Week 5 | Total |
|---|---|---|---|---|---|---|
| joint/ligament | 3 | 6 | 7 | 2 | 0 | 18 |
| stress fractures | 1 | 2 | 2 | 1 | 0 | 6 |
| tendon | 3 | 2 | 3 | 0 | 0 | 8 |
| muscle | 0 | 2 | 1 | 1 | 0 | 4 |
| Total | 7 (19.5%) |
12 (33.3%) |
13 (36.1%) |
4 (11.1%) |
0 (0.0%) |
36 (100%) |
An interesting observation in the present study is that injuries progressively increased in the first three weeks and decreased in the fourth and fifth weeks (Figure 1). Specifically, in week 1, seven injuries affected 19.5% of the total. In week 2, there were 12 that affected 33.3% of the total, and in week 3, 13 injuries affected 36.1%. In week 4, there was a decrease; four injuries (11.1%), and in week 5, there were no injuries. A similar occurrence of injuries in the first two weeks was presented in a study of Greek Army cadets. Although injuries decreased in the last two weeks, it was observed that the cadets had pain and discomfort, mainly in the legs, although they did not visit a doctor as they stated that the BMT was coming to an end.
During the program’s implementation, no allergies or skin conditions were caused by the clothing, even though the military uniform was heavier than the sportswear. Wearing the combat uniform caused more sweat retention because the body breathes less than when in sportswear. In addition, an expected effect of the MT group’s clothing was increased body temperature and heart rate. However, there was no incident of injury or reduced participation in exercise that was solely due to clothing.
Injuries appeared on the lower part of the body, and the leading cause of these injuries appears to be footwear. More specifically, the boots worn by the MT group weighed 1.5 ± 0.25 kg, while the sports shoes worn by the AT group weighed 0.45 ± 0.05 kg. The use of heavy footwear is associated with load carriage11, and previous studies have shown that the average increment in energy cost was 1.0% per 100 gm increase in weight per pair of footwear.
The use of military boots in our study seems to be the factor associated with the increased risk of injury. Although combat boots are designed to protect the foot13, heavy boots may have caused a change in kinematic or mechanical parameters and were related to muscle activation patterns during running, especially at the initial stage of BMT. It seems that the use of military boots in our study compared to sports shoes functioned as a large external load and increased the risk of injury on the lower body. In addition, military boots do not seem to absorb the ground reaction forces during training.
Owing to the small sample size of the present study, compared to other studies4, we cannot claim that the difference in the injuries of the two groups is due to the military combat uniform and boots. A possibility arises that the MT group is exposed to high forces or high loading rates during running with a specific type of boot that is associated with the occurrence of injuries. Then, an intervention that could reduce the risk of injury would be to increase the cushioning in footwear or the design of the training program. The main purpose of BMT is to help the cadets to develop their physical condition and mental/ psychosomatic condition. When these two factors are involved, we should carefully decide what we have to improve first and what needs gradual improvement. We know that extrinsic factors, such as total mileage and training intensity18,19 have also contributed to injury risk. In addition, training programs with adequate training loads are proposed to reduce the risk of injury and produce high fitness. Moreover, if we expect that this period, especially the first five weeks, is sufficient to achieve a relative improvement in aerobic capacity then high intensity interval training (HIIT) programs are suggested to cause metabolic adjustments in just six sessions over two weeks.
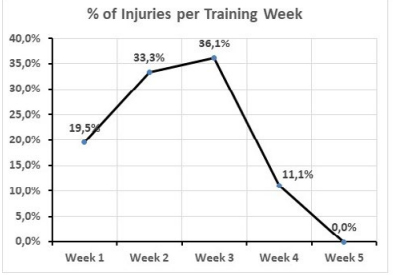
Figure 1. Percentage of injuries per training week
We must agree that BMT, is an initial step in the entire process of training civilian recruits to become effective military personnel, and completing BMT is mandatory for all recruits to progress their career within the military. The results agree that the recruits enter the military with widely varying fitness levels, even within one platoon and confirm that overuse injuries are the most common sustained by military recruits. Injuries, specifically overuse injuries in military recruits during BMT, place a huge logistical and financial burden on military organizations while large increases in training load may precede injury.
Previous research has identified multiple risk factors for training-related injury. For example, the physical fitness components, such as aerobic endurance, muscular endurance, muscular strength, body composition, flexibility, mobility, dynamic balance and asymmetries, appear to increase injury risk.
The increased injury rates lead us to the conclusion that the initial level of fitness of cadets should be assessed and intense activities with military clothing should be avoided to decrease burden. It may be necessary to redefine the exercise program and take more time to adjust the cadets by mainly focusing on their initial fitness level prior to BMT.
When developing training for the Greek Naval cadets, we must create intelligent programs to reduce injuries. As coaches, we must be convinced that the officer we have to prepare for military training, especially during this period, must be treated as an athlete starting their initial training. Subsequently, we need every recruit to be in the training field, not recuperating in a medical office.
The BMT period should generally be treated as an initial stage of training and not as a period in which we monitor the expected problems arising from injuries. Each military unit undertaking the BMT must improve and avoid repeated mistakes that reduce training time and waste money on medical interventions. So we have not made an enormous discovery in BMT; we are just reluctant to change and afraid to improve. We should probably allow for more time to adapt to the desired level set by the requirements of each army. If fitness training is synchronised with military exercises during the BMT period, fewer injuries are likely to occur.
There should be a combination of various activities in BMT, such as running, callisthenics, obstacle course, resistance training, military self-defence, rope climbing and loaded marches. Participating in all these activities elicits large fluctuations in training loads instead of a single activity with a constant moderate training load.
It is important to delimit the exercise and training that needs to be done in the BMT period and to realise that during this period, there are two different types of training, namely sports and military. Sports training aimed at improving fitness should follow the training principles and be separate from the burden of exercise with military clothing. This is probably the key point because it shows that training with military clothing, especially in the first stage of BMT, puts an additional strain on the body. Therefore, the principles of progressive resistance and the gradual increase in volume and intensity must be applied to sports and military training. Sports athletes and military recruits share similarities since both populations strive to achieve high-performance levels. Therefore, a successful military trainer can design a short-term training program to optimise training adaptations and reduce training load error, injuries and attrition.
A consistent moderate training load level can be established through routine monitoring and is suggested to be protective against injury.
Consequently, individualisation and differentiation in training programs are presumably needed to improve the fitness of all recruits to align with military training.
From the specific recording of injuries in the BMT period, it was noted that when the exercise is performed in military combat uniform and boots, there is an increase in injuries. The injuries caused are not only due to the burden of the exercise but also to the added load of clothing with military combat uniform and boots. Those who intend to participate in BMT may need a preparation program to improve their physical condition. BMT can be more functional if the military combat uniform and boots are used as long as the programs are carefully designed so as not to cause unnecessary injuries.
More specifically, the ways to reduce the risk of overreaching or overtraining and provide solutions to optimise training adaptations and reduce injuries in BMT are likely to be (a) the gradual increase of physical fitness without large increases in training load, (b) the prior physical activity levels can be established, and cadets can be categorised into groups according to initial physical fitness, (c) training with groups based on risk factors, (d) carefully planned training load, monitoring load and (e) meticulous choice of clothing and especially footwear.
Conclusion
This study aimed to record injuries following the same kind of exercise with and without military combat uniform during five weeks of BMT in Greek naval cadets. The results showed that the burden of exercise during BMT, which is carried out in military combat uniform and boots, caused several injuries compared to sportswear. Ways to avoid injury can include a carefully designed exercise program according to the principles of coaching, the gradual increase of intensity and total volume, as well as a gradual and staggered introduction to military clothing and footwear. In addition, the initial level of fitness of the Naval cadets in the entry stage of the BMT should also be considered, and the exercise programs should be as carefully designed as possible.
Future studies on the duration of BMT and training programs would provide further information on how to avoid injuries.
Limitations
The findings of this study have the following limitations. Firstly, it concerns Greek Naval cadets accepted into the Hellenic Naval Academy after passing the PanHellenic National University Exams. Secondly, the study did not consider and assess the initial physical condition of the cadets, and the program was not designed accordingly. Thirdly, specific injuries during assessment, for example, those of joints and ligaments, were assessed as one.