
Introduction
The Australian Army’s 1st Brigade is based in Darwin and has a high readiness posture in line with extant requirements. The units of the Brigade include tank, armoured reconnaissance, medium artillery, and combat engineer regiments as well as a mechanized infantry battalion, a combat service support battalion and a command support unit. Individuals posted to the brigade are expected to maintain their readiness status by participation in active physical fitness and battle fitness training and regular field deployments.
A previous paper showed that the Corps a member was serving in was in was not related to the likelihood of downgrading. This report examines the causes of being medically downgraded while serving in the 1st Brigade.
Aim
The aim of this paper is to report the findings of the 1st Brigade Medical Employment Classification Study for the period May 2000 to Apr 2001 as related to the causes of medical downgrading in the Brigade. This paper comes from the data collected as part of the 1st Brigade Medical Employment Classification (MEC) Study. The study protocol was submitted to the then ADF Medical Ethics Committee (now the Australian Defence Human Research Ethics Committee) and was allocated Protocol Number 228/00.
Method
Data was collected on members who met the following criteria:
-
- A member of 1 Bde
An MEC of less than 1 in the period Jan 99 to the date of medical board confirmation
| EPITRACK Event | EPITRACK Code | 1 BDE Code | 1 BDE Event |
|---|---|---|---|
| Intestinal Infectious Diseases | 11 | 1 | Intestinal Infectious Diseases |
| Sexually Transmitted Diseases | 2 | 2 | Sexually Transmitted Diseases |
| Other Infectious and Parasitic Diseases | 3 | 3 | Other Infectious and Parasitic Diseases |
| Malaria | 31 | ||
| Dengue | 32 | ||
| Alcohol and Drug Abuse | 4 | 41 | Alcohol-Related illness |
| 42 | Tobacco-related presentation | ||
| 43 | Substance Abuse- all other | ||
| Mental Disorders | 5 | 53 | Mental Health- all others |
| Stress Reaction | 51 | 51 | Acute Stress or anxiety |
| 52 | PTSD | ||
| Eye Disorders | 6 | 61 | Refraction Check |
| 62 | Eye Disease- all other | ||
| Disorders of the Ear Nose and Throat | 7 | 7 | Disorders of the Ear Nose and Throat |
| Upper Respiratory Tract Infections | 81 | 81 | Upper Respiratory Tract Infections |
| Lower Respiratory Tract Infections | 82 | 82 | Lower Respiratory Tract Infections |
| Diseases of the Teeth and Oral Cavity | 9 | 9 | Diseases of the Teeth and Oral Cavity |
| Diseases of the Digestive System | 11 | 11 | Diseases of the Digestive System |
| Gynaecological (incl Pregnancy) | 12 | 121 | Pregnancy Test |
| 122 | PAP Smear | ||
| 123 | 0 and G- all other | ||
| Ezcematous Skin Conditions | 131 | 131 | Ezcematous Skin Conditions |
| Other Dermatological Conditions | 132 | 132 | Skin- all other |
| 133 | Fungal Skin Infections | ||
| Disorders of the Knee | 14 | 141 | Knee pain |
| Note: The inclusion of these two codes grouped with knee is an anomaly in the Bde coding system compared to EPITRACK. These correspond to EPITRACK Code 16 | 142 | Shin pain | |
| 143 | Leg pain- all others | ||
| Disorders of the back | 15 | 15 | Disorders of the back- no specific injury |
| Other musculo-skeletal diseases | 16 | 16 | Musculo-skeletal diseases- all other |
| Complications of medical care | 17 | 17 | Complications of medical care |
| Other Diseases/ Conditions | 18 | 18 | Other Diseases/ Conditions |
| Injuries due to RTA | 19 | 19 | In juries due to RTA |
| Injuries due to military training | 20 | 201 | Injuries due to PT |
| 202 | Iniuries due to field exercises | ||
| 203 | Army training- all other | ||
| Injuries due to all sport | 21 | 211 | Army organised sport |
| 212 | Sport- all other | ||
| Injuries due to hostile action | 22 | 22 | Injuries due to hostile action |
| Other injuries not due to RTA, training, sport or hostile action | 23 | 231 | All other injuries not covered by other events- on duty |
| 232 | All other injuries not covered by other events- off duty | ||
| Climatic Injury (Heat or Cold) | 24 | 241 | Heat injury |
| 242 | Cold injury | ||
| NBC Indicators | 25 | 25 | NBC Indicators |
| MEC at Entry to Study | MEC at End of Study Period | |||||||
|---|---|---|---|---|---|---|---|---|
| Cause | Total | MEC2 | MEC3 | MEC4 | MEC1 | MEC2 | MEC3 | MEC4 |
| Other infectious diseases | 2 | 2 | 1 | 1 | ||||
| Alcohol abuse | 1 | 1 | 1 | |||||
| PTSD | 1 | 1 | 1 | |||||
| Other mental health | 9 | 6 | 3 | 3 | 6 | |||
| Eye disease | 4 | 2 | 2 | 2 | 2 | |||
| ENT | 7 | 6 | 1 | 5 | 1 | 1 | ||
| Lower Resp Tract | 6 | 4 | 1 | 1 | 5 | 1 | ||
| GI Illness | 8 | 3 | 3 | 2 | 1 | 4 | 1 | 2 |
| Pregnancy | 10 | 10 | 10 | |||||
| Knee Pain | 54 | 10 | 41 | 3 | 4 | 17 | 23 | 10 |
| Shin pain | 20 | 20 | 2 | 6 | 10 | 2 | ||
| Leg pain – others | 14 | 5 | 9 | 2 | 6 | 4 | 2 | |
| Back pain | 57 | 13 | 42 | 2 | 7 | 18 | 22 | 10 |
| Musculoskeletal | 11 | 1 | 10 | 1 | 3 | 5 | 2 | |
| Iatrogenic | 1 | 1 | 1 | |||||
| Medical | 17 | 10 | 16 | 1 | 5 | 10 | 10 | 2 |
| MVA | 18 | 1 | 16 | 1 | 1 | 3 | 11 | 3 |
| PT injury | 31 | 1 | 29 | 1 | 4 | 7 | 17 | 3 |
| Field training | 2 | 1 | 1 | 1 | 1 | |||
| Army training | 4 | 4 | 1 | 1 | 2 | |||
| Army Sport | 30 | 1 | 29 | 9 | 7 | 14 | ||
| Civilian sport | 4 | 4 | 1 | 1 | 2 | |||
| Other injury on duty | 14 | 3 | 11 | 2 | 5 | 7 | ||
| Other injury off duty | 7 | 7 | 1 | 2 | 4 | |||
| 342 | 61 | 264 | 17 | 42 | 103 | 148 | 49 | |
The MEC system in described in DI(G) PERS 16-15 and DI (A) PERS 159-11.2. The approach used within 1st Brigade to the application of the MEC system can be summarized as:
- MEC Class 1 indicates the member is fully fit and healthy, has no restrictions on physical activity and there is no reason to expect the person is more likely to become a casualty than the average soldier.
- MEC Class 2 equates to someone who is able to fulfil their role in an operational or field environment. can train for and pass the majority of components of the standard physical training tests (including the combat fitness assessment). They, however, either require restrictions on the day to day physical training activities or they have a condition that means they are more likely to become a casualty than the average soldier, but the condition can be reasonably managed in the operational environment.
- MEC Class 3 is used where an individual has an unstable condition that cannot be managed reasonably in an operational environment or they have a medical condition that precludes them reaching or maintaining the minimal acceptable physical standards. They are not suitable for deployment to the field however their condition requires further treatment or time before a definitive decision on their outcome is made.
- MEC Class 4 indicates that the person has a condition that precludes them in the long term from operational or field deployments in their current trade. In effect this usually means the individual will be discharged medically not fit for further service.
The medical data detailed in this report was collected by the author in conjunction with the confirmation of medical boards performed on Brigade personnel. Data collection was undertaken between from the start of May 2000 to the end of Apr 2001. Data included:
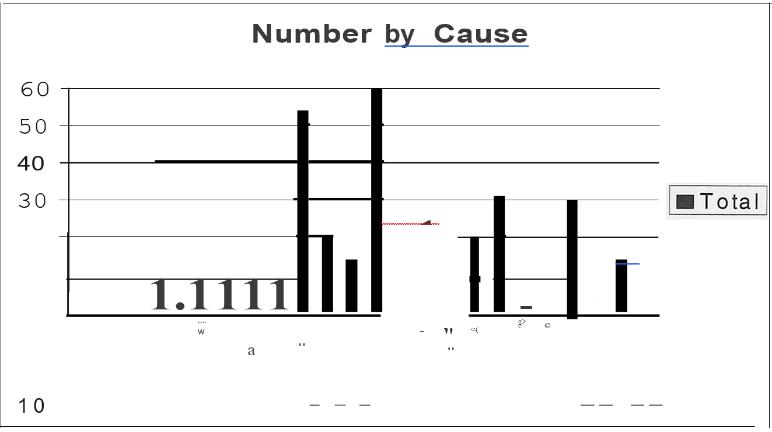
Figure 1: Number of people entered in study by cause of downloading
- Demographic details, including date of birth, whether a transfer from the Ready Reserve of General Reserve streams, current Unit, corps and employment category number (ECN).
- Clinical details, including diagnosis leading to downgrading, chronological summary of condition, whether formal surgical intervention has occurred and whether the member has undergone a formal rehabilitation program.
- Medical board details, including date and result of significant medical boards (usually the initial or transfer medical board, the medical board where downgrading occurred and the latest medical board) and height and weight measurement recorded on the medical board.
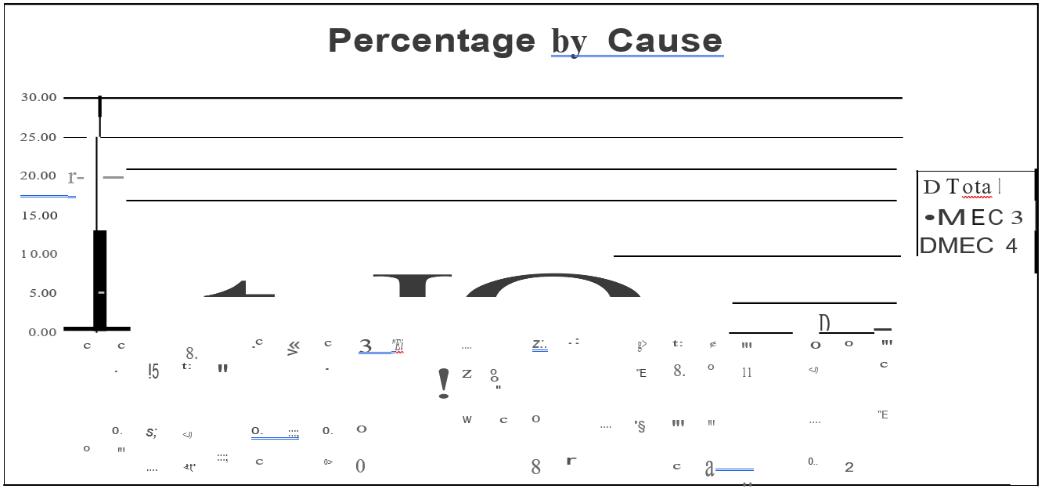
Figure 2: Cause of downgrading as percentages – Total and for outcomes MEC 3 and MEC 4
The diagnosis in each case was coded by the author using the 1st Brigade Health Surveillance Codes. These are based on the EPITRACK codes as used in the Australian Defence Force Health Surveillance System3.4 with local modification for greater detail resolution in some areas. Table 1 lists the EPITRACK codes and the corresponding 1st Brigade codes. The 1st Brigade codes will be used throughout this article.
| Outcome | Total | MEC 1 | MEC 2 | MEC 3 | MEC 4 |
|---|---|---|---|---|---|
| Back Pain | 21.89 | 2.79 | 7.16 | 8.75 | 3.18 |
| Knee Pain | 20.29 | 1.59 | 6.76 | 9.15 | 2.79 |
| PT Injury | 11.94 | 1.59 | 2.79 | 6.76 | 0.80 |
| Army Sport/td> | 11.94 | 3.58 | 2.79 | 5.57 | 0.00 |
| Medical | 10.35 | 1.99 | 3.98 | 3.98 | 0.40 |
| Shin Pain | 7.96 | 0.80 | 2.39 | 3.98 | 0.80 |
| MVA | 6.76 | 0.40 | 1.19 | 4.38 | 0.80 |
| Other Leg Pain | 5.57 | 0.80 | 2.39 | 1.59 | 0.80 |
| Other Injury on Duty | 5.17 | 0.80 | 1.59 | 2.79 | 0.00 |
| Musculoskeletal | 4.38 | 0.40 | 1.19 | 1.99 | 0.80 |
| Pregnancy | 3.98 | 0.00 | 0.00 | 3.98 | 0.00 |
| ENT | 2.79 | 0.00 | 1.99 | 0.40 | 0.40 |
| G1 Illness | 2.79 | 0.40 | 1.59 | 0.80 | 0.00 |
| Other Injury Off duty | 2.79 | 0.40 | 0.80 | 1.59 | 0.00 |
| Other Mental Health | 2.39 | 0.00 | 0.00 | 1.19 | 1.19 |
| Lower Retract | 1.99 | 0.00 | 1.99 | 0.00 | 0.00 |
| Army Training | 1.59 | 0.40 | 0.40 | 0.80 | 0.00 |
| Civilian Sport | 1.59 | 0.40 | 0.40 | 0.80 | 0.00 |
| Other Infectious Disease | 0.80 | 0.00 | 0.00 | 0.40 | 0.40 |
| Eye Disease | 0.80 | 0.00 | 0.80 | 0.00 | 0.00 |
| Alcohol Related | 0.40 | 0.40 | 0.00 | 0.00 | 0.00 |
| PTSD | 0.40 | 0.00 | 0.00 | 0.00 | 0.40 |
| Iatrogenic | 0.40 | 0.00 | 0.00 | 0.00 | 0.00 |
| Field Training | 0.40 | 0.00 | 0.00 | 0.40 | 0.00 |
| Total | 129.33 | 16.71 | 40.59 | 59.29 | 12.73 |
In recording the cause of injuries, a review of the member’s medical documents was conducted to ascertain the nature of the activity at the time of injury. Where possible the distinction was made between injuries that arose during physical training activities and those that arose during formal Army organised sport. Where injuries arose from sport played as part of physical training, this was recorded. Where it was not possible to tell if the activity was physical training or formal sport, it was recorded as sport.
The Chi-Squared test was used to determine the significance of the results (p<0.05).
Results
Table 2 shows the number of people at each MEC at entry to the study by cause and the ‘outcome’ (the MEC at the end of Apr 2001). Two diagnostic categories (back pain and knee pain) were the cause of downgrading in 111 out of the 342 members in the study (32.4%). Figure 1 shows the total number of people in the study by cause.
Figure 2 shows the causes of downgrading as a percentage of the number of people downgraded in comparison to the relative contribution each cause makes to the outcome of MEC 3 and MEC 4. The cause of downgrading members in the study was back pain in 19.92% and knee pain in 15.69% of cases. These two conditions accounted for 25% and 21.88% of MEC 4 cases in the study (p=0.01). Army sport was the cause of 9.23% of various conditions in people in the study; however, it led to no members being classified MEC 4 and was responsible for 21.93% of those that recovered to be MEC 1 (p=0.001). Table 3 shows the rate per 1000 of each cause for downgrading by MEC.
Selected Categories
The causes and outcomes of the four codes with the largest numbers were examined.
| Cause | Number |
|---|---|
| Idiopathic/ no cause recorded | 39 |
| Spondylolithsesis | 5 |
| MVA/MBA | 6 |
| CFA | 3 |
| Battle PT | 2 |
| Jump or fall of truck | 2 |
| Lifting at work | 2 |
| Ankylosing Spondylitis | 2 |
| PT | 1 |
| S 12 ort- Ruby | 1 |
Back Pain
The majority of the back-pain patients coded as Code 15 (back pain) had low back pain (55 out of 57). The diagnosis recorded for each member in the study was searched and it revealed a total of 63 patients with low back pain as their diagnosis. Where there was an acute injury associated with their back pain, these patients were coded according to the mechanism of injury. Table 4 shows the causes of low back pain and Table 5 shows the outcome for these patients. The numbers are too low to determine any significant difference.
| MEC Outcome | MEC 1 | MEC 2 | MEC 3 | MEC 4 |
|---|---|---|---|---|
| Total number | 8 | 18 | 24 | 13 |
| Number that had rehab | 8 | 3 | 21 | 6 |
| Number that had operation | 1 | 3 | 1 | 1 |
Knee Pain
There were a total of 42 patients in the study with a knee problem. These included people with knee pain without acute injury and those who had an acute injury that lead to their knee pain. There were 28 anterior cruciate ligament (ACL} injuries in the study. The commonest causes of these were PT and Australian Rules (4 each) followed by rugby and soccer (3 each). 5 of the 28 patients with ACL recovered to be MEC 1, 9 recovered to be MEC 2 and the remaining 14 are still MEC 3. No patient was discharged during the period because of their ACL injury. It should be noted that a number of the members who were still MEC 3 had been so for over 18 months and may eventually have an outcome of MEC 4
| MEC Outcome | MEC 1 | MEC 2 | MEC 3 | MEC 4 |
|---|---|---|---|---|
| Total number | 3 | 8 | 22 | 9 |
| Number who had TIT | 3 | 5 |
There were a further 42 patients in the study with a diagnosis of either chondromalacia patella or patellofemoral arthralgia. For the majority of these patients, no clear relationship could be established from their Unit Medical Record between the knee pain and particular activity. Table 6 shows the outcome and the number of patients who underwent tibial tubercle transfer (TIT) procedures.
PT Injury and Army Sport
Table 7 shows the physical training activity being undertaken when acute injuries occurred as recorded in the member’s medical records. The knee was the most commonly injured part (17 out of 32) during physical training activities, with the shoulder being the next most common (5 out of 32). Table 8 shows the sport associated with a downgrading injury. The commonest part injured during sport was the knee (18 out of 28). With the ankle (4 out of 28) and shoulder- (3 out of 28) next most common.
| Activity | Number |
|---|---|
| Not recorded | 9 |
| Battle PT | 6 |
| Run jump dodge course | 6 |
| Touch (not organised sport) | 4 |
| Running | 2 |
| Basketball | 2 |
| Other | 3 |
| Sport | Number |
|---|---|
| Australian Rules | 7 |
| Rugby | 6 |
| Soccer | 6 |
| Basketball | 3 |
| Netball | 2 |
| Other | 4 |
Shin Splints
22 patients were downgraded for shin splints or compartment syndromes. Only two patients associated their shin splints with marching, the remainder with running. 12 of the 22 underwent fasciotomies. Of those who did not have fasciotomies, one recovered to MEC 1, 3 to MEC 2 and one became MEC 4. Five are still undergoing treatment. Of those who had fasciotomies, one recovered to MEC 1, four to MEC 2, six are still undergoing management and one was made MEC 4. The numbers are too low to determine significance.
Discussion
Rudzki and Cuningham5 looked at wastage rates and training programs in initial training establishments. The medical discharge rate in their study was 47/1000 for males and 164/ 1000 for females in 1995/1996. They do not indicate the different causes of medical discharge and the aim of their study was to examine the effect of changes to a training program in injury rates. The population in the 1 Bde study was trained soldiers with varying lengths of service and hence the results are not comparable.
Bergman and Miller-6 reviewed medical discharges from the British Army between 1861 and 1998 in the context of prevailing community disease rates. They report a medical discharge rate related to injury in 1998 of 2.8 per 1000. In the 1 Bde study the medical discharge rate for injury-related conditions was 8.36 per 1000. The study methodologies are different and the definition of an injury used by Bergman and Miller is not clearly spelt out but the results are suggestive of a much higher career-ending injury rate in 1 Bde than in the British Army.
Low back pain is the leading cause of both downgrading and medical discharge in this study, with a high percentage of those with back pain being discharged medically unfit. It is noteworthy that of the 8 members with back pain who became MEC l, 7 had been placed on a formal rehabilitation program whereas only 6 out of 13 who had an outcome of MEC 4 had been placed on a rehabilitation program. This result is worthy of further examination. It may indicate that there is a group of patients with low back pain that the medical officer felt was not going to do well even with rehabilitation and hence they were not referred. It may, however, represent an access issue in that there was no rehabilitation program in operation, or it was operating at a reduced rate, during the period these members were being assessed. The number of people with low back pain and its association with medical discharge indicate that consideration should be given to developing a standardized approach to determining those at risk in order to prevent the condition developing.
The outcome of members with knee pain strongly suggest that members who require a tibial tubercle transfer do not do well with respect to recovering to a deployable standard. This needs further investigation as in some cases the procedure may have been done early in their military career and they had in fact ‘soldiered’ on for some years before their condition worsened.
Physical training activities are a major source of lost workdays according to the ADF Health Status Report. It is difficult to draw any comparisons between the data in the Health Status report and this study because of the different sources of data as well as the different coding and terms for diagnosis. Both show that the lower limb is at particular risk form physical training activities. With this study showing the knee to be the body part which most correlates with physical training and sporting injuries that lead to downgrading.
In this study, the distinction is made between sport played as part of physical training and sport played in organised army competitions. This reveals that touch football played as part of physical training led to 4 members being downgraded but no members suffered a downgradable injury as a result of organised touch competitions.
There are a number of obvious differences between the two situations, including standard of play, enforcement of rules, motivation and activity prior to playing. It is not known if the data presented in the ADF Health Status report was able to distinguish between organised competition and sports played as part of physical training. It would seem that this distinction may be relevant with respect to the relative risk of the activity.
In this study, no member was found to be medically unfit for further service as a result of an injury sustained during Army sporting competitions. The reasons for this are not apparent from the data in this study. It may represent the impact of these injuries occurring in a more motivated group of individuals, earlier presentation and optimum management including adequate rest and rehabilitation or a willingness to ‘persevere’ longer with their treatment rather than discharge them earlier. A number of members in this category were still MEC 3 at the end of the period and this result may be misleading.
The outcomes of members who had fasciotomies for shin splints and those who did not does not suggest there is any real difference. The numbers, however, were low and hence firm conclusions cannot be drawn on this issue from this study.
Conclusion
Medical discharge associated with back pain, knee pain, physical training, and shin pain accounted for approximately 60% of medical discharges. This wastage could be reduced by implementation of injury prevention programs, development of screening methods for those at risk of back, knee and shin pain, and the development of improved treatment regimens. At the core of such programs is refined surveillance of presentations to medical facilities, and outcomes of injuries over time, to provide data across the ADF with which to identify causal and associated factors in career-ending injuries and preventable conditions.



