
Introduction
The Australian Army’s 1st Brigade is based in Darwin and has a high readiness posture in line with extant requirements. The units of the Brigade include tank, armoured reconnaissance, medium artillery, and combat engineer regiments as well as a mechanized infantry battalion, a combat service support battalion and a command support unit. Individuals posted to the brigade are expected to maintain their readiness status by participation in active physical fitness and battle fitness training and regular field deployments.
Members of the Australian Army are assigned to Corps based on their trade or professional skills. These Corps can be grouped according to their role in combat into combat (RAAC, RAA, RAINF and AAVN), combat support (RAE, RASIGS and Aust Int) and combat service support corps (the remaining). All units of the Brigade have members from a number of different corps. The combat and combat support units are comprised primarily of soldiers belonging to the relevant Corps (for example, the infantry battalion has primarily soldiers from the Royal Australian Infantry (RAINF) corps).
Given the disparate nature and environment of the work in each unit, ranging from working in and around armoured vehicles, mechanized infantry soldiering, combat engineering, field artillery work, to operational logistic support (warehousing, driving, maintenance and health support), it might be expected that certain Corps are more likely to be associated with being medically downgraded than others. This paper examines the hypotheses that service in certain Corps of the Army is associated with a higher likelihood of being medically downgraded.
Aim
The aim of this paper is to report findings of the 1st Brigade Medical Employment Classification Study for the period May 2000 to Apr 2001 as related to the Corps of the individual. A subsequent report will examine the causes of downgrading in the Brigade. This paper is derived from the data collected as part of the 1st Brigade Medical Employment Classification (MEC) Study. The study protocol was submitted to the then ADF Medical Ethics Committee (now the Australian Defence Human Research Ethics Committee) and was allocated Protocol Number 228/00.
Method
Data was collected on members who met the following criteria:
- A member of 1 Bde
- A MEC of less than 1 in the period Jan 99 to the date of medical board confirmation.
The MEC system is described in DI(G) PERS 16-15 and DI (A) PERS 159-11.2. The approach used within 1st Brigade to the application of the MEC system can be summarized as follows:
- MEC Class 1 indicates the member is fully fit and healthy, has no restrictions on physical activity and there is no reason to expect the person is more likely to become a casualty than the average soldier.
- MEC Class 2 equates to someone who is able to fulfill their role in an operational or field environment, can train for and pass the majority of components of the standard physical training tests (including the combat fitness assessment); however, they either require restrictions on day to day physical training activities or they have a condition that means they are more likely to become a casualty than the average soldier, but the condition can be reasonably managed in the operational environment.
- MEC Class 3 is used where an individual has an unstable condition that cannot be managed reasonably in an operational environment or they have a medical condition that precludes them reaching or maintaining the minimal acceptable physical standards. They are not suitable for deployment to the field; however, their condition requires further treatment or time before a definitive decision on their outcome is made.
- MEC Class 4 indicates that the person has a condition that precludes them in the long term from operational or field deployments in their current trade. In effect, this usually means the individual will be discharged
The data detailed in this report were obtained from:
- Data related to the distribution of personnel by Corps in the Brigade came from Brigade Documents of the Brigade Units.
- Data related to the MEC status of Brigade personnel was obtained from the 1st Brigade Medical Readiness Database. This provides a point in time ‘snap shot’ of the health status checks of its accuracy against the source documents (an individual’s unit medical record). Checks have revealed approximately 5% of the members of the Brigade have not been entered on the database and 5% of the members on the database have left the Brigade. The data used in the report were taken on the author’s final days in the Brigade prior to posting.
Medical data was collected by the author in conjunction with the confirmation of medical boards performed on Brigade personnel. Data collection was undertaken between from the start of May 2000 to the end of April 2001. This included:
- Demographic details, including date of birth, whether a transfer from the Ready Reserve of General Reserve streams, current Unit, corps and employment category number (ECN).
- Clinical details, including downgrading diagnosis, chronological summary of condition, whether formal surgical intervention has occurred and whether the member has undergone a formal rehabilitation program.
- Medical board details, including date and result of significant medical boards (usually the initial or transfer medical board, the medical board where downgrading occurred and the latest medical board) and height and weight measurement recorded on the board.
The Chi Squared test was used to determine the significance of the results (p< 0.05).
Results
A total of 342 members of the brigade were entered into the study during the 11 months of data collection covered by this report.
| Corps | Total in Bde | MEC 2 | MEC 3 | MEC 4 | Total in Study |
|---|---|---|---|---|---|
| RAAC | 423 | 4 | 37 | 2 | 43 |
| RAA | 138 | 3 | 19 | 0 | 22 |
| RAE | 236 | 8 | 16 | 3 | 27 |
| RASIGS | 168 | 3 | 30 | 1 | 34 |
| AAAVN | 28 | 1 | 1 | 0 | 2 |
| RAINF | 468 | 4 | 29 | 5 | 38 |
| AAINT | 14 | 0 | 1 | 0 | 1 |
| RACT | 163 | 3 | 27 | 1 | 31 |
| AACC | 82 | 2 | 10 | 0 | 12 |
| RAAMC | 66 | 3 | 12 | 2 | 17 |
| RAAPsycb | 3 | 0 | 0 | 0 | 0 |
| RAADC | 18 | 1 | 3 | 0 | 4 |
| RAAOC | 287 | 13 | 33 | 2 | 48 |
| RAEME | 354 | 12 | 36 | 0 | 48 |
| RACMP | 37 | 1 | 6 | 0 | 7 |
| RAAPC | 19 | 1 | 2 | 1 | 4 |
| AALC | 2 | 0 | 1 | 0 | 1 |
| RAACHD | 4 | 2 | 1 | 0 | 3 |
| Totals | 2513 | 61 | 264 | 17 | 342 |
Table 1: MEC at Entry to study by Corps
Table 1 shows the Medical Employment Classification at entry into the study against the member’s Corps. The table includes the total number of people in the Brigade from each Corps at the start of the study. Figure 1 compares the percentage of people in the Brigade from each Corps and the percentage of people in the study from each Corps. There is no significant difference between the percentage of the Brigade in each Corps and the percentage by Corps of members in the study.
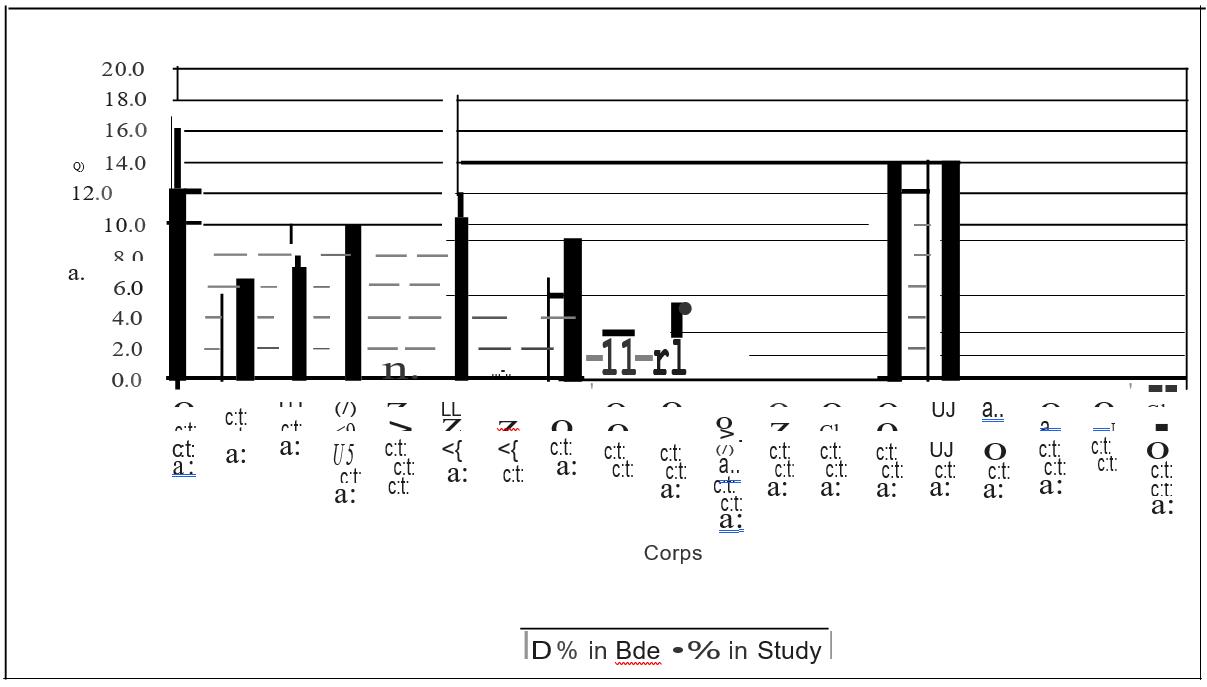
Figure 1: Comparison of percentage of members of the Brigade in each Corps and the percentage in the study in each Corps
Of the 61 cases where the member was MEC 2 on entry to the study, 56 of them remained MEC 2 throughout the study period. indicating that their condition had stabilised in the medium term at a level consistent with deployment. Of the five who did not remain MEC 2, two were upgraded to MEC 1, two were downgraded to Class 4 and one was Class 3 at the end of the study period.
| Corps | Total |
|---|---|
| AAVN | 1 |
| RAA | 3 |
| RAAC | 4 |
| RAACHD | 2 |
| RAAMC | 3 |
| RAAOC | 13 |
| RAAPC | 1 |
| RACMP | 1 |
| RACT | 3 |
| RAE | 8 |
| RAEME | 13 |
| RAINF | 3 |
| RASIGS | 3 |
| TOTAL | 61 |
Table 2 shows the number of members who entered the study of MEC 2 by their Corps.
| Codes | Class 1 | Class 2 | Class 3 | Class 4 | Total |
|---|---|---|---|---|---|
| AAVN | 1 | 1 | |||
| AACC | 1 | 3 | 4 | 2 | 10 |
| AustINT | 1 | 1 | |||
| AALC | 1 | 1 | |||
| RAA | 1 | 3 | 11 | 5 | 19 |
| RAACHD | 1 | 1 | |||
| RAADC | 1 | 2 | 3 | ||
| RAAMC | 2 | 10 | 12 | ||
| RAAOC | 4 | 6 | 20 | 3 | 33 |
| RAAPC | 1 | 1 | 2 | ||
| RACMP | 2 | 4 | 6 | ||
| RACT | 4 | 4 | 16 | 3 | 27 |
| RAE | 5 | 4 | 6 | 1 | 16 |
| RAEME | 4 | 7 | 22 | 3 | 36 |
| RAINF | 4 | 4 | 20 | 1 | 29 |
| RASIGS | 5 | 5 | 18 | 2 | 30 |
| Total | 40 | 46 | 148 | 30 | 264 |
Table 3: MEC 3 at entry, by outcome and Corps
Table 3 shows the cause of downgrading by Corps for the 264 members who entered the study as MEC 3 and their outcome at the end of the study period.
| Corps | Number |
|---|---|
| RAAC | 2 |
| RAAMC | 2 |
| RAAOC | 2 |
| RAAPC | 1 |
| RACT | 1 |
| RAE | 3 |
| RAINF | 5 |
| RASIGS | 1 |
| Total | 17 |
Table 4: MEC 4 at entry to study by Corps
Table 4 shows the Corps for the 17 members who entered the study as MEC 4. All these individuals have been discharged or are awaiting discharge.
| Combat | CS | CSS | |
|---|---|---|---|
| Total | 42.06 | 16.63 | 41.31 |
| Stucil | 33.10 | 17.79 | 49.11 |
| 1 | 38.46 | 23.08 | 38.46 |
| 2 | 31.11 | 17.78 | 51.11 |
| 3 | 29.93 | 17.01 | 53.06 |
| 4 | 42.55 | 14.89 | 42.55 |
Table 5: Percentage of Bde by Corps Grouping and Outcome
Table 5 compares the percentage of people in the Brigade in the Corps groups (combat. combat support and combat service support) and their representation in the study by outcome. There are a significantly higher percentage of members of the CSS corps in the ‘still MEC 3’ group (p=0.03). The percentage of members of the CSS Corps that had an outcome of MEC 2 was high but did not reach significance (p=0.07).
| Corps | Bde | All | 1 | 2 | 3 | 4 |
|---|---|---|---|---|---|---|
| RAAC | 16.8 | 13.9 | 25.6 | 17.8 | 8.2 | 19.1 |
| RAA | 5.5 | 6.8 | 2.6 | 4.4 | 7.5 | 10.6 |
| RAE | 9.4 | 6.8 | 10.3 | 8.9 | 4.1 | 8.5 |
| RASIGS | 6.7 | 11.0 | 12.8 | 8.9 | 12.2 | 6.4 |
| RAINF | 18.6 | 12.1 | 10.3 | 8.9 | 13.6 | 12.8 |
| RACT | 6.5 | 10.0 | 10.3 | 8.9 | 10.9 | 8.5 |
| RAAOC | 11.4 | 12.5 | 10.3 | 13.3 | 12.9 | 10.6 |
Table 6: Percentage of personnel in the Bde and in the Study by Corps who were MEC 3 or 4 on entry to study against outcome.
Table 6 shows the percentage of personnel in the Brigade by Corps, MEC 3 or 4 on entry to study and outcome. There was a significant difference between the number of members from each corps in the study and the number that had an outcome of Class 1 (p = 0.01) and Class 3 (p = 0.02). The difference between the members by Corps in the study and those who had a Class 4 outcome was close to significant (p=0.06).
Discussion
According to the Australian Defence Force Health Status Report3, as at January 1999:
- 92.9% of Australian Regular Army (ARA) personnel had a classification of MEC 1 or MEC 2 as of January 1999
- 2.9% of the ARA was Class 3,
- 1.7% was Class 4, and
- 2.5% had no classification.
According to the 1 Bde medical readiness database, as at July 2001.
- The percentage of the Bde who were MEC 1 or 2 was 94.7%,
- 4.3% of the Bde was MEC 3, and
- 1% of the Bde was MEC 4.
The differences are not significant.
There is no data available on downgrading by Corps in other Army formations. Anecdotally, one might expect the Combat Arms Corps to have a higher percentage of downgrading based on the need to achieve a relatively high level of fitness and the inherent nature of their routine activity, making it harder for someone with any chronic injury or condition to maintain such a standard. The results indicate that, in the 1st Brigade, the likelihood of medical downgrading is not dependent on the Corps a member is serving in. One explanation for this is that the rate of physical training and activities is similar across all units in the brigade. Of note is the difference in outcome by Corps. The significant differences in Table 6 are related to:
- A higher percentage of RAAC and RASIGS members who had a Class 1 outcome.
- A lower than expected percentage of members from RAA and RAINF who had a Class 1 outcome.
- The higher than expected percentage of RASIGS and All other Corps who were Class 3 at the end of the period.
- The lower than expected percentage of RAA and RAINF members who were Class 3 at the end of the period.
The results suggest that it is harder for members of the RAA and the ‘minor’ Corps (shown as ‘all other’) to regain Class 1 status after a downgrading event. It is worth noting that these two groups were also overrepresented in the Class 4 outcome.
There are numerous factors that have not been taken into account in this study. These include:
- The effect of different medical officers conducting the medical boards. The use of a confirming authority and an algorithmic approach to determining medical classification should negate some of this effect.
- The impact of transfers between Corps (noting that Corps at time of initial injury or illness diagnosis was not recorded).
- The effect of different Corps serving in different Units.
Conclusion
The identification of risk factors for medically downgrading is a key step in minimizing the loss of personnel. In the 1st Brigade, it would appear that the member’s Corps is not a significant risk factor. The difference in outcome between Corps is worthy of further investigation to determine the reasons for this finding. Other factors of potential significance, which have not been examined in this study, include the corps and unit of the member at the time of initial injury or diagnosis and the time between onset of condition and downgrading.



