
Abstract
Military prison camps have historically been terrible places with excessive mortality. A review of extant records from the 19th to the 20th century indicates that gastrointestinal mortality dominated in both cold weather and tropical prison camps. Malnutrition and gastrointestinal infections became mutually re-enforcing causes of mortality in prison camps, including Andersonville, Georgia, during the US Civil War, French prisons in Guyana and New Caledonia, British colonial government of India prisons in the Andaman Islands, Finnish and Japanese prisoner of war (POW) camps during World War II and US camps for Chinese/Korean POW during the Korean War. Overall mortality ranged from 6% to 33%, with a majority due to diarrhoea and dysentery. Crowded camps with poor sanitation and inadequate water supplies were the worst in terms of survival. Historical horror stories are in danger of repetition during modern crises if simple field sanitation cannot be instituted and maintained.
As these waters, loaded with filth and human excrement, flow sluggishly through the swamp below, filled with trees and reeds, coated with a filthy deposit, they emit an intolerable and most sickening stench.
Dr Joseph Jones 18651
Military prison camps with crowded and unsanitary conditions have often become focal points of increased mortality due to diarrhoea and dysentery. This has been especially true for prisoner of war (POW) camps, which were overcrowded with surrendered personnel forced into a bare existence with inadequate food and water supplies. That this existed during the US Civil War in 1864 is not historically surprising as it was before the understanding of the microbiological nature of infectious diseases. Still, similar dysfunctional camps with lethal consequences existed well into the 20th century. Disease disasters during armed conflict and refugee movements could reoccur today if basic principles of field hygiene are ignored. The ancient Roman Army understood that latrines and mess facilities needed to be physically separated within the camp, even if they did not understand anything about bacterial contamination of food and water sources. Historical examples from the USA, French, British, Finnish and Japanese military experiences regarding prisoner mortality due to gastrointestinal infections are reviewed.2,3,4,5,6,7 The selection of examples largely depended on those historical instances with extant data in English. Mortality risk primarily reflected logistical issues of crowding, poor nutrition, unsafe water sources and inadequate field sanitation.
Most soldiers during the US Civil War died of infections, not combat. ‘Did not have the guts to be a soldier’ originally referred to the gastrointestinal tract, not any perceived act of cowardice.8 The Confederate prison camp at Andersonville, Georgia, was the worst example of what could happen when previous government-sponsored parole agreements broke down, supplies fell short due to the Union shipping blockade and medicine was incredibly basic due to scientific ignorance.9 Figure 1 indicates the exceedingly crowded conditions in the POW camp with primitive field hygiene facilities. It is estimated that 13 000 of 45 000 Union prisoners (28%) died at Andersonville, mostly over 14 months 1864–65.10 Hospital and burial records indicate that the vast majority of deaths were due to malnutrition (vitamin deficiencies such as scurvy) and diarrhoeal infections.1, 10 Figure 2 show the estimates of causes of death in the Andersonville prison camp. Dr Joseph Jones, the military medical officer who investigated the mortality crisis for the Confederacy, knew that the primary problem was the halt in prisoner exchanges due to political disagreements and the inadequacy of supplies due to the Union blockade.1 These harsh wartime realities did not stop post-war accusations of war crimes, eventually leading to the execution of the Andersonville camp commandant.1 Crowding large numbers of prisoners into a small area without clean water or field sanitation was a disaster that extracted an enormous mortality tax on the prisoners.

Figure 1: Photo of USA Union Army soldiers at the Andersonville, Georgia prison camp showing the crowded conditions under improvised shelters with field latrines (sinks) in the foreground that led to thousands of prisoner deaths due to gastrointestinal infection. Photo by AJ Riddle in 1864 via the National Parks Service (https://www.nps.gov/media/photo/gallery-item.htm). Now in the public domain.
Not all prison camps were for POW; France sent civilian convicts to colonial prisons in both Guyana in South America and New Caledonia in the Pacific in the latter half of the 19th century. Despite the similarities between the prisoners exiled overseas and the general conditions of servitude in French camps, the mortality rates in the two prison colonies were very different. Malaria and yellow fever were endemic in Guyana and absent from New Caledonia. Between 1–3% of prisoners died annually of diarrhoea or dysentery3 (see Figure 3). Diarrhoeal deaths were much higher in New Caledonia from midcentury despite the overall mortality being 50% greater in Guyana due to the additional infectious disease burden primarily due to malaria. For comparison, dysentery mortality rates from the British colonial government of India’s prison camps on the Andaman Islands are included in Figure 3 as another area with endemic malaria.5 By 1880, all three prison camps’ diarrhoeal disease mortality rates had moderated, likely due to efforts to improve field hygiene and faecal disposal practices.3, 5 Diarrhoeal diseases and subsequent mortality were always worse when the camps were being organised or after a large influx of new prisoners likely due to inability to have field sanitation and water facilities ready from the beginning.
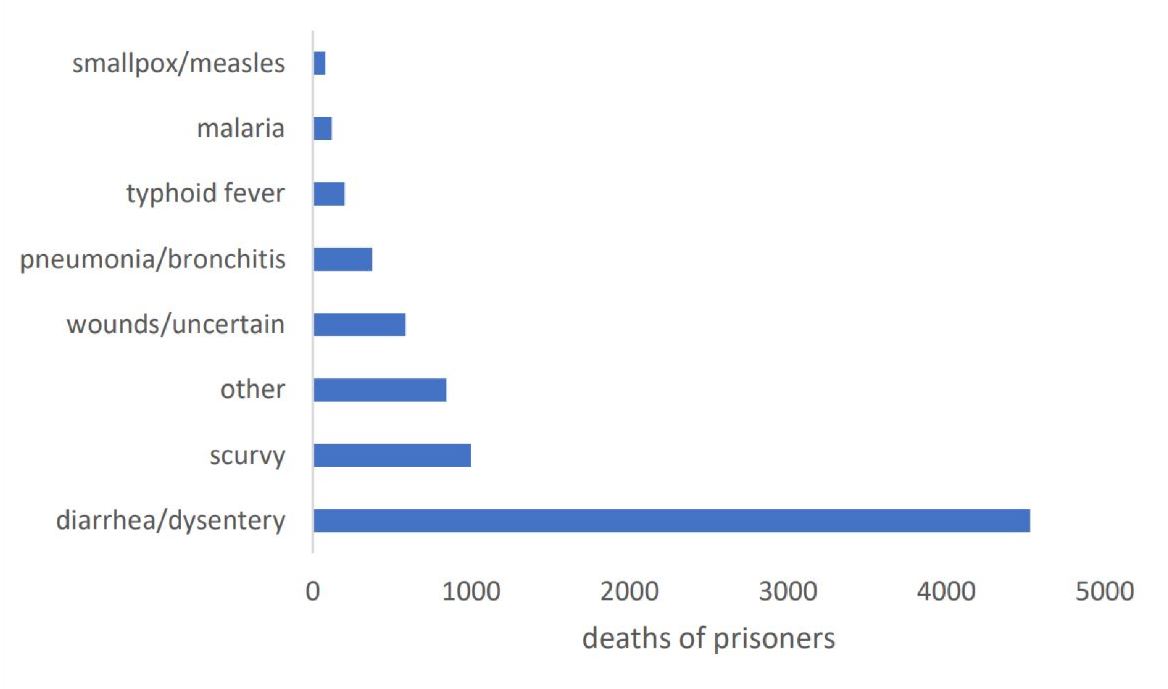
Figure 2: Causes of death of USA Union Army soldiers at the Andersonville, Georgia prison camp in 1864–65 based on reports of Confederate medical officers working at the prison hospital and post-war burial records. 13 000 (28%) of the 45 000 Union soldiers confined at Andersonville died largely of gastrointestinal infections and malnutrition.1, 9, 10
World War I had several examples of prison camp mortality due to gastrointestinal disease. The Australian Imperial Force at Gallipoli was little more than an open prison camp, given the limitations of space, lack of fresh water and poor sanitation facilities during a siege inside a small coastal enclave encircled by the Turkish Army. Dysentery and diarrhoea were the leading infectious disease problems of Gallipoli, requiring many to be evacuated to Malta in the preantibiotic era.11 Over a quarter of a million Italian POW were captured just after a single battle (Caporetto) in 1917, forming part of >600 000 Italian POW incarcerated by the Austro-Hungarian Empire.12 Diarrhoeal disease was the leading cause of death, with an estimated 17% of captured soldiers not surviving the war. However, detailed quantitation across the main camps was unavailable.
POW camps during World War II included the infamous camps of Allied prisoners along the Thai–Burma railway 1942–45, where most deaths resulted from a combination of malnutrition (beriberi), diarrhoeal diseases and malaria.4, 13 Cholera epidemics killed many along the railway in 1943.14 Roughly 1:4 of the 60 000 POW did not survive the war, with the leading listed cause of death was dysentery.15 A valuable comparison to what was experienced on the Thai–Burma railway can be made with Soviet POW and civilians held in Finnish camps during 1939–44, where about 1:3 of the 64 000 prisoners did not survive the war6 (see Figure 4). This was despite the ethnic Russians in Finland not being involved in forced labour projects. Malnutrition (largely starvation) and diarrhoeal diseases were the leading causes of death. The added complication of severe cold during winter was another significant loss of calories in addition to the war-restricted food supplies.6 Malaria was present but not a major cause of death.16 Cold temperatures may have limited the spread of enteric infections seasonally. Still, the overall death rates due to diarrhoeal diseases were high, with moderation over the course of the war. Differentiation between malnutrition, malabsorption and enteric infection was impossible as these were largely symptomatically indistinguishable and likely formed a spectrum of disease manifestations.6
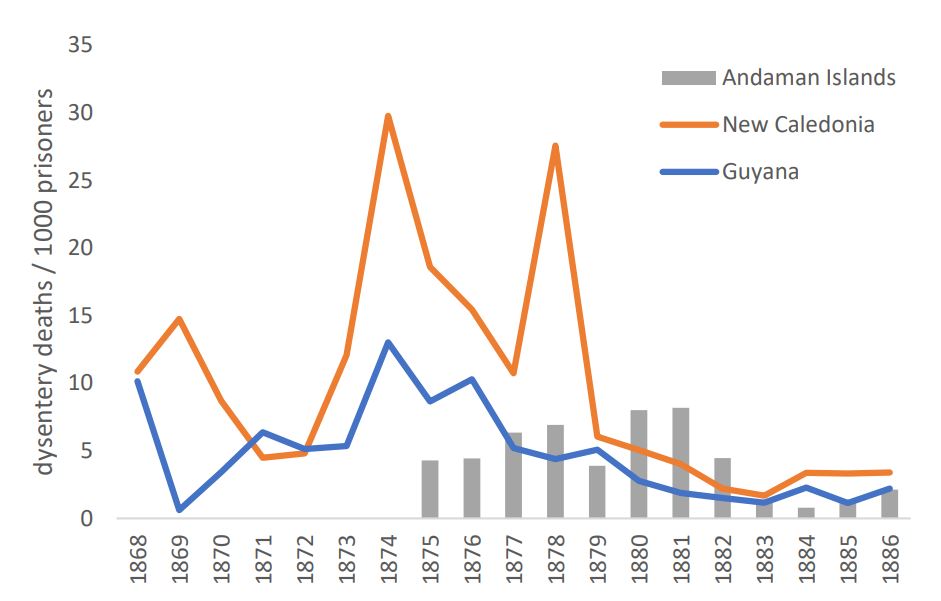
Figure 3: Dysentery mortality rates in French civilian prisoners at camps in Guyana and New Caledonia 1868-1886 based on French medical officers’ reports.3 Similar information from the British colonial government of India prison camps on the Andaman Islands 1875–1886 with dysentery mortality is shown for comparison.5
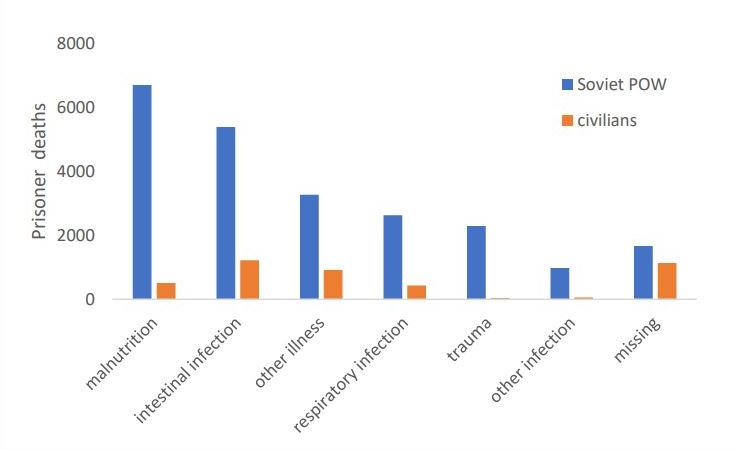
Figure 4: Causes of death in Russian (Soviet) POW and civilian internees in Finland during the winter and Continuation Wars of 1939–1944. Approximately one-third of Russian prisoners captured in Finland (total=64 000) did not survive the war, most dying of gastrointestinal infections and malnutrition.6
One can expect acute health problems anytime a large population of unwilling prisoners without much understanding of field sanitation are rapidly collected into POW camps. This occurred in the aftermath of the Chinese People’s Liberation Army intervention during the Korean War 1950–53.7 Relatively few Chinese/Korean prisoners died in US POW camps, with a mortality rate of 5.8% out of 132 474 registered POW administered in camps controlled by the USA military.7 Dysentery (likely Shigellosis) was the leading killer in 1950, even after the advent of the antibiotic era (see Figure 5). Tuberculosis reactivation was an important secondary cause of death that prevailed after diarrhoeal diseases had been controlled by better POW administration and camp management.7 The Korean War POW experience is essential in pointing out that even well-resourced military groups can have difficulty managing field sanitation in large numbers of POW camps.
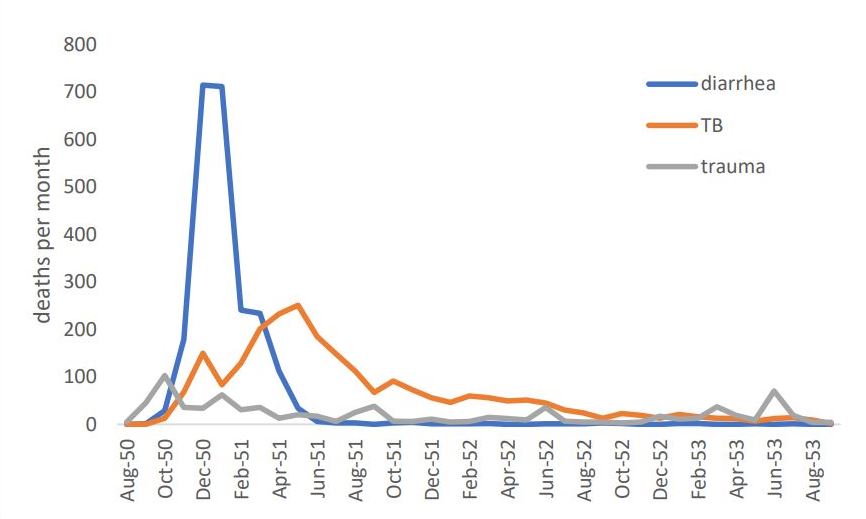
Figure 5: Deaths in US prison camps during the Korean War 1950–53 in Korean/Chinese POW (total=132 474), of which 5.8% died in captivity mostly of gastrointestinal causes and reactivation tuberculosis.7
Although there is a tendency to see such prison camp mortality crises as a dark and distant history, continuing armed conflicts in parts of the developing world suggest otherwise. The Rwandan War of 1994 and the associated genocide produced large numbers of refugees in what was then known as Zaire (now Democratic Republic of the Congo). Although the initial concern focused on a cholera epidemic, drug-resistant Shigella dysenteriae was the cause of many deaths in the Goma refugee camps.17 The campsite consisted mainly of a lava field with no natural water sources, which only complicated the sudden need to provide field sanitation for more than a million people. In future Humanitarian and Disaster Relief (HADR) missions that the Australian Defence Force may be tasked to respond to minimise mortality, it is essential to get basic field sanitation done correctly at the beginning of the crisis.11 There are distinct limitations to using historical casualty data derived under the stress of war and disaster, so one has to realise the approximate nature of the recorded information. Although cultural practices apply in different civilian or military populations, the practical medical need to separate food, water and faeces leaves some non-negotiable factors that must be solved in field sanitation when large numbers of people are suddenly confined in camp areas. Current military medical officers must recognise the difficulties of field sanitation during future wars and humanitarian disaster relief missions.
Corresponding Author: G D Shanks, Dennis.Shanks@defence.gov.au
Authors: G D Shanks1,2
Author Affiliations:
1 ADF Malaria and Infectious Disease Institute
2 University of Queensland – School of Public Health



