
Abstract
Background: Injury prevention contributes to the improvement of basic military training graduation rates.
Purpose: To obtain an estimated effect of agility training (AT) on body control, change of direction speed (CODS), and attrition due to injuries in Dutch recruits. Methods: Cluster randomised pilot study including 64 recruits undergoing 23 weeks initial military training with the Air Manoeuvre Brigade. Recruits performed the T test and Illinois Agility Test (IAT) pre- and post-intervention (week 6 and week 19) to evaluate body control and CODS. After 23 weeks we evaluated injury attrition rates.
Results: Recruits in the AT group had on average 0.17 seconds faster T test times than recruits in the control groups (CG) (95% CI:-0.48 to 0.13); and on average 0.14 seconds faster IAT-times (95% CI:-0.40 to 0.12), adjusted for baseline scores. Relative risk (RR) of attrition due to injuries in the first six weeks was 1.81 (95% CI 0.32 to 10.11, p=0.65), while that from week 6-23 was 0.32 (95% CI 0.12 to 0.85, p=0.018).
Conclusion: This pilot study provides preliminary evidence that AT may help retain body control and CODS and may reduce attrition due to injuries.
Key Words: Agility training, change of direction speed, armed forces, injury prevention
Introduction
Alertness and manoeuvrability can be a matter of life and death for combat troops. Military service demands a variety of physical abilities, such as carrying heavy loads over long distances and rough terrain, sprinting and employment of military operations in urban environments. The speed at which these activities are performed can affect a soldier’s fighting effectiveness and combat survivability. Maximum physical performance in these environments requires, among other things, strength, speed, agility, and aerobic and anaerobic endurance3,8,12,13,14,23,25.
Approximately 1500 men and women aged 17-27 years, volunteer for service in the Netherlands Armed Forces (NAF) each year. Of these, about 200 undergo training with the 11 Air Manoeuvre Brigade (11 AMB), a rapid response infantry unit that can be deployed anywhere worldwide within 7-20 days. 11 AMC’s Basic Military Training (BMT) program lasts
23 weeks, including 11 weeks’ basic military training and 12 weeks’ advanced airmobile infantry training. The need for a high BMT graduation rate is driven by cost-effectiveness considerations and reduced injury rates. Although reducing the intensity and frequency of training could be a logical strategy, this is at odds with the imperative to deliver highly competent infantry soldiers to the units, who are physically and mentally prepared for combat operations.
The United States (US) Army’s Joint Physical Training Injury Prevention Working Group (JPTIPWG) recommends that multiaxial, neuromuscular, proprioceptive and agility exercises be included as a regular component of military physical training programs. Among its other findings, the JPTIPWG obtained moderate evidence that increasing the proportion of physical training time for exercises that vary musculoskeletal stress in multiple planes, such as agility training (AT), reduces injury risk2. Agility is defined as ‘a rapid whole body movement with change of velocity or direction in response to a stimulus’27. The reactive component includes cognitive functions, such as visual processing, timing, perception and anticipation while the action is an open motor skill, which cannot be pre-planned. Therefore, agility drills teach the brain how to control the body when reacting to a stimulus. By focusing on specific cues, agility drills help improve and correct body position, balance, coordination and explosive movement patterns5. It has been suggested that improved agility also includes increased body control
during fast movements, increased intramuscular coordination and decreased risk of injury or reinjury7,19,22. However, AT is not yet structurally programmed in the current physical training programs in the NAF.
The results of a recent study of 41 subjects at the US Air Force School of Aerospace Medicine suggest that six weeks of AT, compared to running and calisthenics, resulted in significant within-group performance improvements in cardiorespiratory capacity and change of direction speed (CODS), as well as sustained attention, and improved accuracy and speed of working memory. In contrast, six weeks of traditional training did not yield such improvements in the control group16. However, a study of a novel training program for trained male soldiers that incorporated AT did not yield relevant improvements to agility17. Likewise, in a study of civilian men undergoing a complex program including AT was not superior to a general program of calisthenics and running for improving performance of five simulated army battlefield activities. Although the volunteers in both study arms improved significantly on all tests, there were no statistical significant differences in training effect between the study arms9. More research is needed to determine how AT should be incorporated in the military training program to achieve the best results. In addition, the feasibility of adapting traditional military training, with its strong focus on military skills training and long distance marches carrying heavy loads, should be assessed.
The primary objective of this pilot study was to obtain an estimated effect of 12 weeks of AT on body control and CODS on 11 AMB recruits compared to the standard 11 AMB physical training program. The secondary objective was to explore the effect of 12 weeks of AT on these recruits, with respect to injury attrition rates.
Methods
This was a cluster randomised controlled pilot study of four BMT classes. On average, 60 recruits start the AMB BMT in each recruiting period, with about of 15 recruits per class. Human Resources divided these before BMT into balanced classes based on age, prior education and future military position after graduation. Classes receive physical training in pairs. Independent from the grouping, we used cluster randomisation to assign the intervention to two of the four classes, which formed the intervention (AT) and control groups (CG). An independent study assistant who drew lots performed randomisation.
The source population consisted of men and women who volunteered to undertake 11 AMB BMT. However, there were no females in this cohort. Eligibility criteria included: age between 17 and 27 years, minimum height 165 cm, minimum weight 65 kg, maximal vision correction of minus 6.0 or plus 6.0, and proof of swimming proficiency. The period of enrolment was January 2015 through July 2015. All BMT candidates were required to pass a preparticipation medical examination and complete a three-day introduction program.
All participants were briefed on the study objectives in week 1 of the BMT by the lead author (ID), both verbally and in writing, and provided written informed consent. The Central Committee of Research of the Netherlands involving human subjects waived the study from formal medical ethical review, noting that the goal of improving (military) physical performance was based on the standard nature of the compared exercise programs.
Procedures
During the first six weeks of the BMT, both groups received the same physical training program, with an emphasis on strength training. In the seventh week, military specific and functional training exercises started for both groups. The physical training time for both groups was 1.5–2 hours per day. The CG received the standard physical training program, supervised by a designated sports instructor, during the whole BMT. This program included running, calisthenics, obstacle course, strength circuits, military self-defence, and wall and rope climbing.
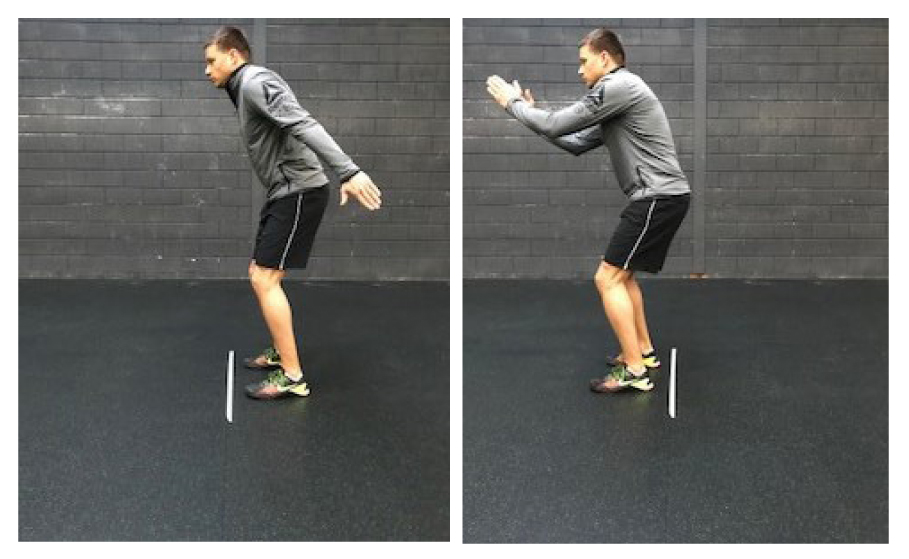
The AT group underwent the standard physical training program for the first six weeks, 20 minutes of which was substituted with 20 minutes of AT three times a week from the seventh week. The first three weeks of the AT program (week 7-9 of BMT) consisted primarily of preconditioning basic skills (basic level), such as lateral and backwards movements and direction changing. Exercises during the second three weeks (week 10-12 of BMT) targeted acceleration, deceleration and more complex changes of direction (intermediate level) while the last six weeks (week 13-18 of BMT) contained reactive and explosive agility drills (advanced level)5. Cues varied between sound, timing, visual and physical stimuli, and became increasingly unexpected and more diverse from week four until week 12. See Appendix 1 and Appendix 2 for details of the agility drills. The training sessions of the AT group were also given by designated sports instructors who had undergone training for the study intervention.
Measurements
Anthropometric measurements were taken in the first week of the BMT, pre-intervention (week 6 of the BMT, denoted T0) and post-intervention (week 19 of the BMT, denoted T1).
Body control and CODs were assessed at T0 and T1 using the T test and the Illinois Agility Test (IAT) by independent study assistants who were blinded for group assignment. Outcome assessors were trained to use the measurement tools prior to any study procedures. The tests demonstrated good reliability and validity for this purpose in a military population22. Times to complete the tests were measured using the Brower Timing System which is accurate to 1/1000 second26. The change from pre- to post-intervention on the CODS and body control tests, measured in 1/100 second, was used as the dependent variable.
Injury attrition rates were evaluated at the end of the 23-week program (denoted as T2). The platoon commander registered dropout-rates and reason for dropout at the moment the recruit was dismissed from the training program
Statistical analyses
Descriptive analysis was used to report anthropometric characteristics of the participants at the start of the BMT, Welch two sample t-tests were used to test for baseline imbalances.
Intention-to-treat analysis of the primary outcome body control and CODS included paired students t-tests to estimate within-group changes, and linear regression analysis with adjustment for the score at T0 to estimate between-group differences. We performed a multilevel analysis to assess the need to account for clustering. This analysis showed no statistically significant intracluster correlation coefficient, and the results were comparable to those of the ordinary least square regression analysis. We therefore present the results of the latter analysis. Results are presented with 95% confidence intervals (CI) and Cohen’s d effect sizes (ES). ES of 0.2 is considered a small effect, 0.5 a medium effect and 0.8 a large effect4.
To explore the effect of AT on attrition due to injuries from week 1 until the end of the BMT, we calculated relative risk (RR) ratios with 95% CI and a corresponding p-value of the Fisher’s exact test. We calculated the RR for the first six weeks of the BMT and additionally, the RR from week six until the end of the BMT (T2). We used R version 3.1.3 for statistical analyses21.
Results
All recruits who started the BMT in October 2015 agreed to be included in the pilot study. Of the 64 recruits who started the BMT in week 1, 53 were still participating at T0 (see Flow chart). The anthropometric characteristics were all comparable at baseline, T0 and T1. The baseline anthropometric characteristics are presented in Table 1. No statistical baseline imbalances were found between the AT and CG. Of the 36 planned AT sessions, 26 (72%) occurred.
Primary outcome:
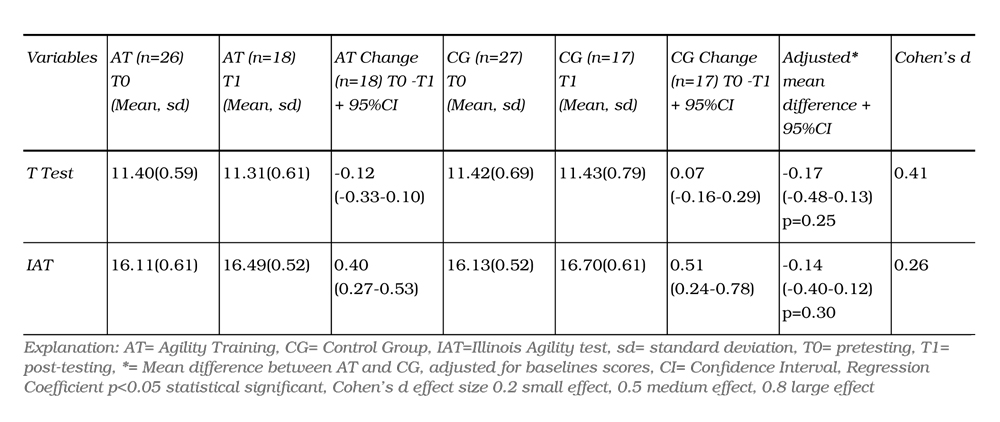
Recruits in the AT group had on average 0.17 seconds faster T test times than recruits in the CG (95% CI: 0.48 to 0.13, Cohen’s d=0.41); and on average, 0.14 seconds faster IAT-times (95% CI: 0.40 to 0.12, Cohen’s d=0.26), adjusted for baseline scores (Table 2).
Secondary outcome:
Thirty-two recruits successfully completed the BMT, 18 of whom (28%) were in the AT group, while 14 (22%) were in the CG. Reasons for withdrawal included injuries (AT:7, CG:15) and requested discharge (AT:4, CG:6). For the AT group, RR of attrition due to injuries in the first six weeks was 1.81 (95% CI 0.32 to 10.11, p=0.65), compared to the CG, while RR of attrition due to injuries from week six until the end of the BMT (i.e. during the experimental period) was 0.32 (95%CI 0.12 to 0.85, p=0.018), and thus statistically significant. Injuries varied by body region and onset (acute vs overuse), and included muscle strains in lower back, shoulder, and leg and knee pain. Reasons for requesting discharge from the BMT included altered career ambitions and lack of motivation.
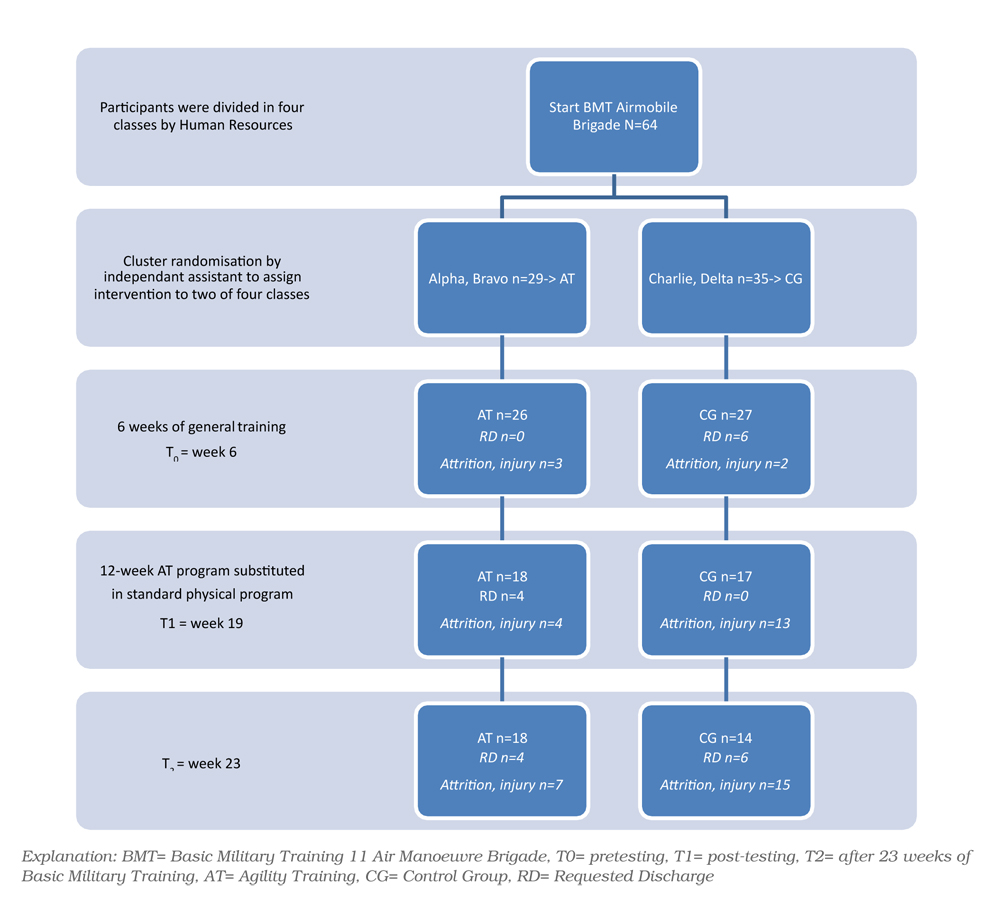
Table 1: Baseline characteristics (week 1 BMT)
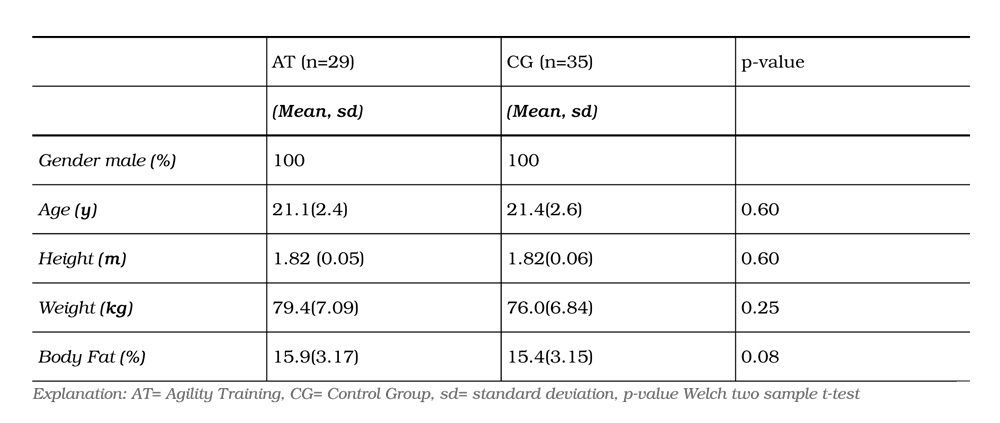
Table 2: Primary results, body control and CODs
Discussion
The objective of this cluster randomised pilot study was to estimate the effect of 12 weeks AT on body control, CODS and injury attrition rates among recruits of the Dutch 11 AMB. This sample demonstrated a limited effect on body control and CODS after 12 weeks of AT integrated in the BMT, favouring the intervention group. This suggests that AT might limit the loss of body control and CODS during initial military training. More importantly, AT resulted in less withdrawal from initial military training for injury compared to the CG group over the length of the 23-week BMT.
Our findings regarding the primary outcome are in agreement with comparable studies suggesting that, although the training effect on body control and CODS—an intermediate outcome—was small, incorporating AT into military training programs could be useful9,16,17. Our study results suggest that even small improvements in these effect–measures, may reduce injury attrition rates among AMB BMT participants. Increased anaerobic endurance and neuromuscular control could have contributed to less muscular fatigue and therefore, lowered the risk of injuries6. Another possible explanation could be that substituting a part of the obstacle course and running training sessions with AT reduced training intensity, thereby resulting in less fatigue and better training adaptation11.
However, there is a great difference between the physiological demands of AT and long distance marches carrying heavy loads with the former improving anaerobic endurance while the latter improves aerobic endurance11. Long distance marches are an essential part of the infantry training and a major component of BMT. The marching program includes a total of 280 kilometres spread over the 23 weeks of the BMT, with a final overnight march of 25 kilometres. In general, the BMT is designed to frequently expose the recruits to uncomfortable circumstances. These become more extreme towards the end of the BMT, culminating in a final field test where exhaustion, sleep deprivation, physical discomfort, and (minor) injuries are common. These extreme circumstances are likely to have affected the performance of the recruits during the AT sessions as well as the performance on pre and post-intervention testing in both groups. The speed of movement and power produced in each agility drill determines the degree of positive adaptations. Subjects should perform all drills with maximum speed and power as anything less decreases the force and power developed, diminishing the training effect27. The recruits may have restrained themselves during both the AT sessions as well as during pre and post-intervention testing out of fear of injuries and subsequent dismissal from the training program.
The JPTIPWG recommends that multiaxial, neuromuscular, proprioceptive and agility exercises should be included as regular components of military physical training programs2. Our results support this recommendation, noting the difference in injury attrition rates (43% in the CG to 25% in the AT), which increased the number of recruits who passed the BMT, rather than being dismissed from the training program. Considering that each recruit already costs about €33.817 at the beginning of the BMT, AT may contribute to improve cost-effectiveness of military training15.
However, this pilot study also revealed some important barriers to implementing AT. Of the 36 planned AT sessions, only 26 of the sessions (72%) were carried out. Cancellation of training sessions occurred mainly in the last three weeks of the program, in both AT and CG, mostly because of scheduling issues. The lack of continuity in training sessions reflects the challenges for implementing AT in the standard physical training program, resulting from time limitations, the large number of goals to be achieved, limited availability of sports instructors and scheduled field weeks.
The strengths of this pilot study are the comparability of the groups concerning demographic characteristics at baseline and performance at the start of the experimental period (T0), and the generalisability resulting from the pragmatic character and protocolled AT training sessions. Furthermore, as we did not want to expose recruits to more physical training than the military training already comprises, the AT group had no extra training time compared to the CG. Finally, the intervention involved reactive drills and starting cues to stimulate anticipation and reaction time to enhance cognitive functions with a view to improving alertness and manoeuvrability. Some weaknesses of the study should also be noted. Although female sex was not an exclusion criterion, the absence of female recruits in this cohort, prevents generalisability of our findings to females. Another limitation of this pilot study is the small sample size, which limited the precision of the effect estimates, especially given the attrition rate before T0. Post-hoc power analysis suggested that the initial sample size was sufficient to show a statistically significant benefit of AT compared to CG of the observed magnitude, on T test times post-intervention. We acknowledge that attrition of BMT as well as the occurrence of musculoskeletal injuries in recruits result from multifactorial processes. A previously proposed multifactorial model of athletic injury aetiology states the interplay between intrinsic factors (e.g. personal factors, previous injury, strength, age), extrinsic factors (e.g. training load, environment) and injury incidence18. Additionally, several researchers recognised the nonlinear interplay between those factors and proposed the ‘web of determinants’, emphasising the complexity of injury risk1,10,20. As this was beyond the scope of our study, we did not measure or address personal factors such as grit or ambition level. However, we believe that the random nature of group assignment likely harmonised the groups on these features. Because of this, and because the attrition rate before T0 was not associated with the intervention (since the intervention had not yet started), we believe that observed RR represent a valid estimation of the effect.
Previous research showed that the training methods and qualification of sports instructors are relevant for recruits’ fitness development in initial military training24. Although, the sports instructors who gave the training sessions to both the AT group as well as the CG were experienced trainers, they had little experience with AT prior to this study. Although provision of the AT program was standardised, technique, intensity, speed, rest and motivational feedback are of great importance to the degree of positive adaptions27. Instructors in this pilot study were working their way through their learning curve in providing AT. This may have influenced the quality of the instructions limiting the intervention effects. Even larger effects may therefore be attainable if sports instructors receive additional schooling in skills as AT for military personnel. The Netherlands has several institutions where such courses are available. We hypothesise that the effects of AT are likely to increase CODS and body control in the field, especially with improved compliance to the program and if sports instructors gain more AT experience. We also consider the development of a tactical reactive agility test to be useful for measuring both physical and cognitive effects of renewed training programs in military populations.
In this pilot study we focused solely on exploring the effects of AT to the standard BMT program on body control, CODS and attrition rates. The addition of interventions to optimise personal factors, as well contextual factors, may further improve the outcomes of BMT. We suggest that future studies should investigate the effectiveness of such multidimensional interventions.
Conclusion
Our study shows that there are challenges in implementing AT in initial military training programs. Despite its limitations, this pilot study suggests that AT may have added value as a standard component in initial military training of Airmobile recruits. Larger trials are needed to confirm these findings. Careful consideration should be given to the planning of AT in relation to the remainder of the military training program, to ensure continuity and consistency of AT training sessions.
Corresponding Author: Iris Dijksma, I.Dijksma.01@mindef.nl
Authors: I Dijksma1,2, S Perry1, W Zimmerman3,4, C Lucas1, M Stuiver1
Author Affiliations:
1 University of Amsterdam
2 Defence Health Care Organisation
3 Royal Netherlands Army
4 Uniformed Services University of Health Sciences
Appendix 1: Intervention, Agility Training
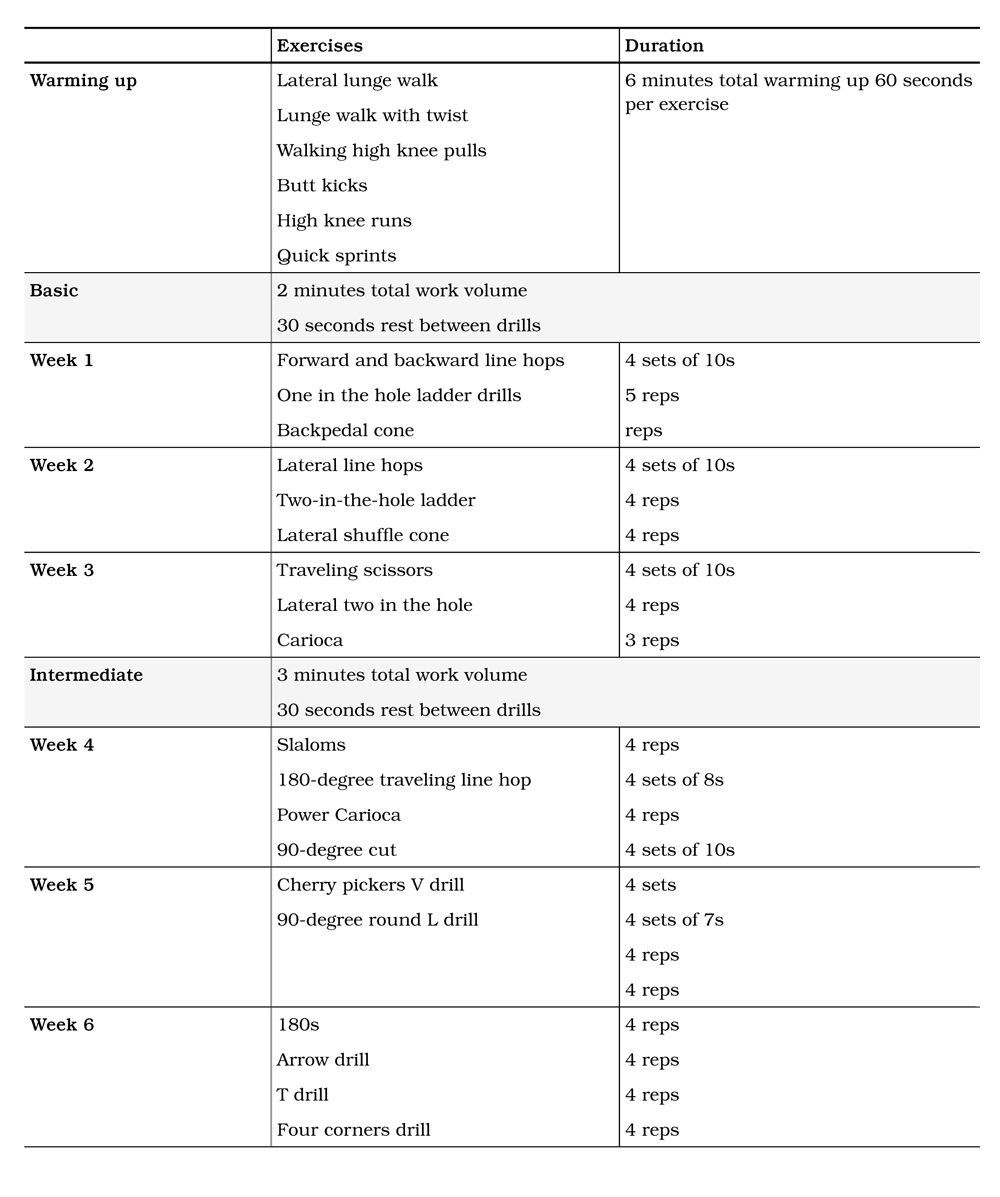
Appendix 2: Selection of agility exercises used in the intervention(14)
Warming up
Lateral lunge walk
Extend the arms in front of the chest, take a big step to the side and bend the knee of the lead leg once the foot touches the ground.
Keep your arms extended throughout the exercise to assist with balance.
Lateral lunge walk with twist

Extend the arms in front of the chest, take a big step forward and flex the knee of the lead leg to approximately 90 degrees. Then rotate your hips and shoulders towards the lead leg. Return to the starting position by stepping forward with your trial leg. Repeat the exercise with the opposite leg.
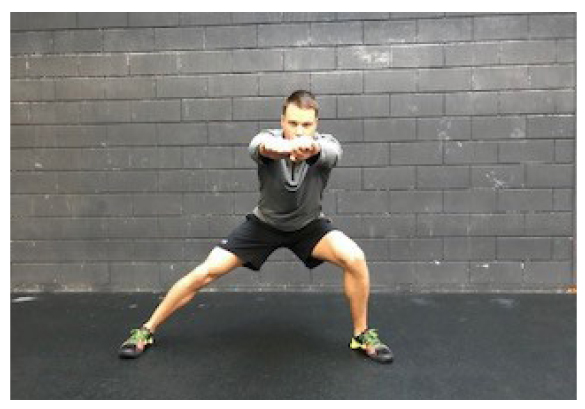
Walking high knee pulls
Start with flexing one hip and lifting your knee on that side as high as possible; grab the leg below the knee and pull your knee to your chest, keeping your back and chest up. Return the raised leg to the ground and repeat while moving forward with the other leg.
Basic
Forward and backward line hops
Stand in an athletic position parallel with the line facing forward and hop as fast as possible back and forth over the line with your feet together.
Lateral line hops
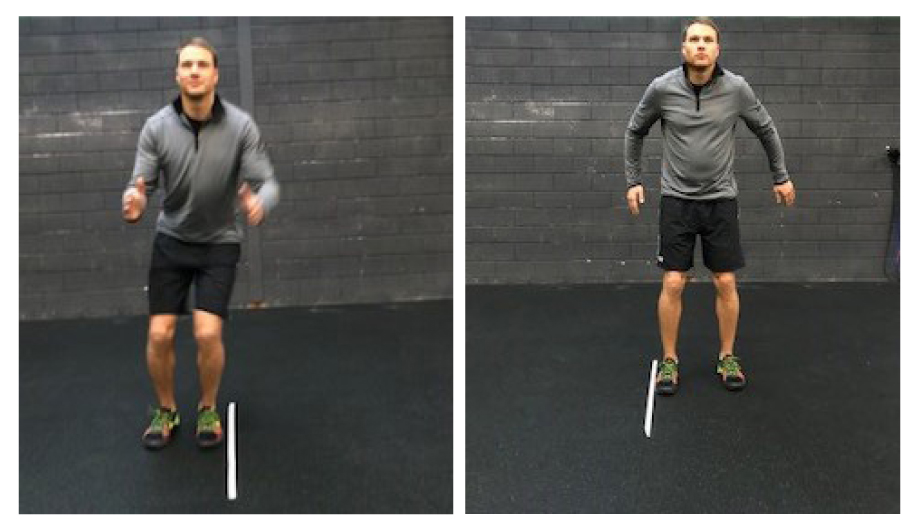
Stand in an athletic position with your shoulders perpendicular to the line and hop as fast as possible sideways over the line with your feet together.
Two-in-the-hole ladder
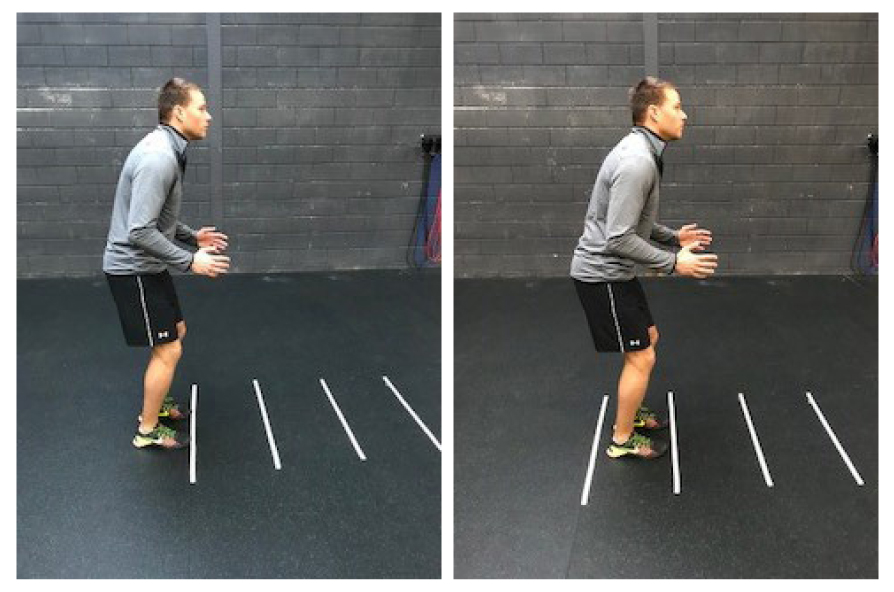
Stand in an athletic position at the end of the ladder facing forward. Step into the first box with one foot and immediately step into the same box with the other foot. Continue this pattern as fast as possible through the ladder.
Intermediate Slaloms
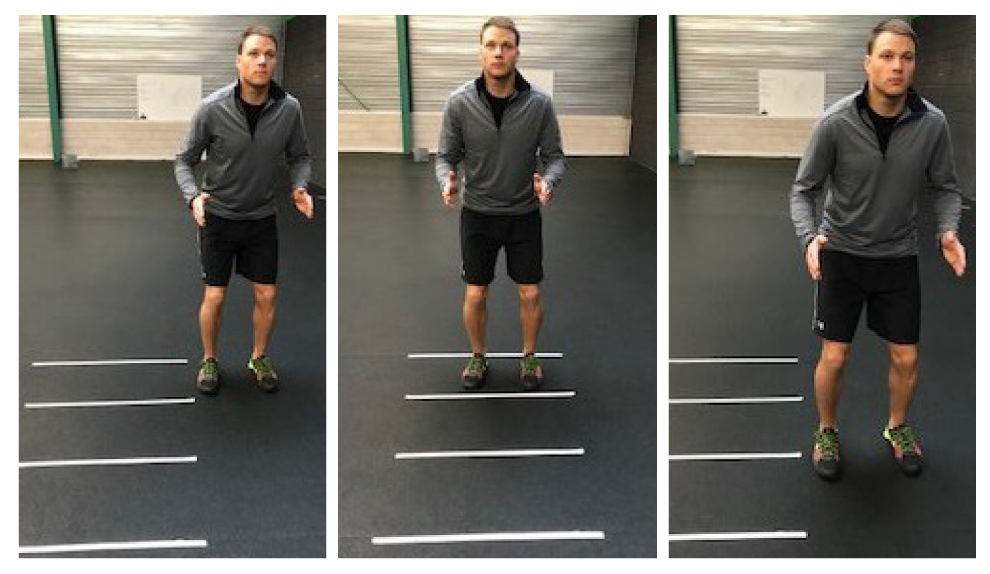
Stand in an athletic position to the side of the first box with your hips and shoulders parallel to the ladder. Hop with both feet tighter into the centre of box 1 and immediately hop out of the box to the other side.
Hop diagonally into the centre of box 2 and immediately hop out of the box diagonally landing at the top of box 2. Continue this zigzag pattern through the ladder.
90-Degree round
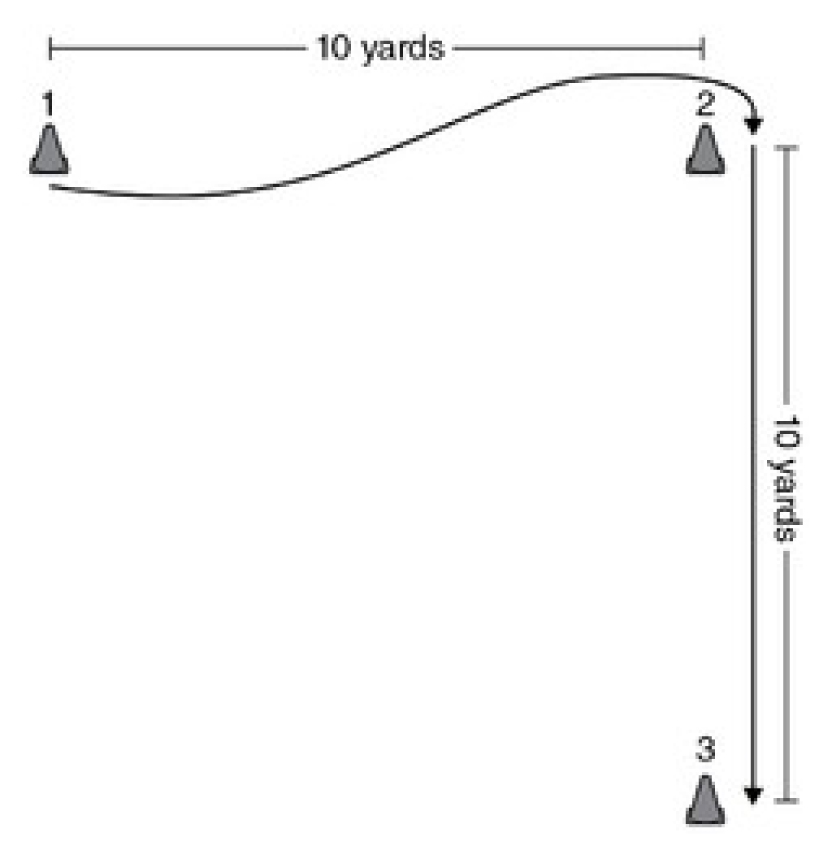
Start next to cone 1 with your hips, shoulders and torso parallel to the cone. Sprint on cue towards cone 2; slow down slightly and make a 90- degree turn around cone 2. Then accelerate and sprint past cone 3.
T drill
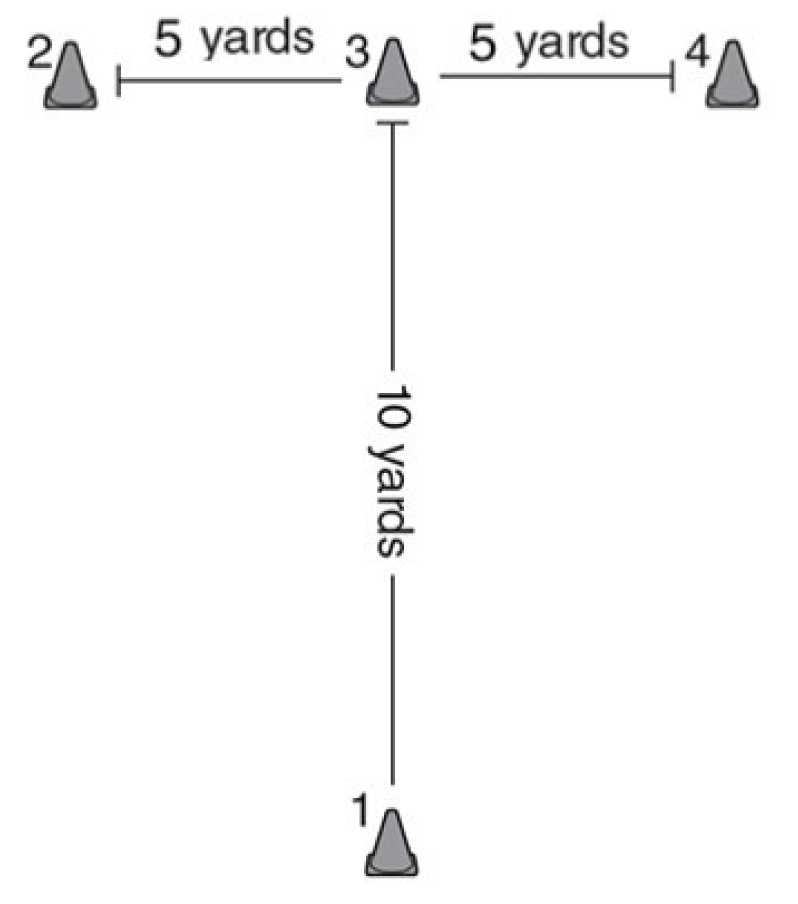
Start in an athletic position at cone 1, sprint to cone 3, cut left and sprint to cone 2. Then, perform a 180-degree turn around cone 2 and sprint to cone 4. Perform a 180-degree turn around cone 4 and sprint back to cone 3, then cut let and sprint back past the starting cone. Use short and choppy steps during the drill.
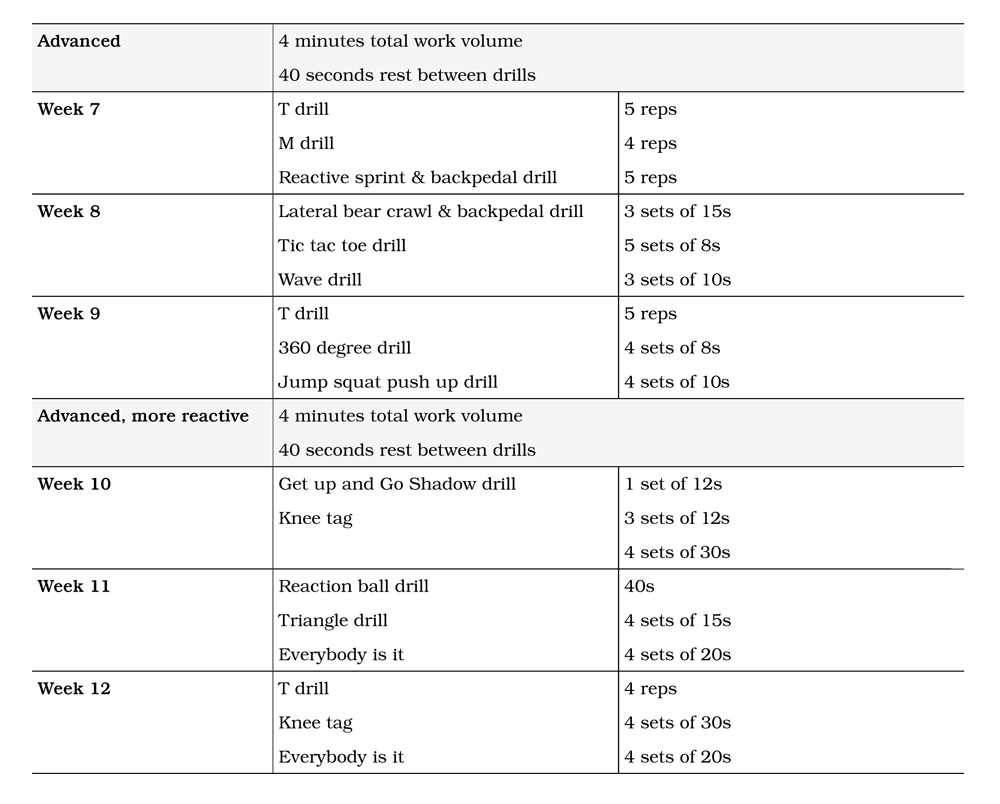
Advanced
Lateral bear crawl and backpedal drill

Set 4 cones in a square with 5 yards between cones. Start in an athletic position on the outside of cone 1 with your hips, shoulders and torso perpendicular to it. On cue, sprint to cone 2. Then, assume a bear crawl position and move laterally to cone 3. Stand up as fast as possible and backpedal to cone 4. Then, bear crawl laterally back to cone 1.
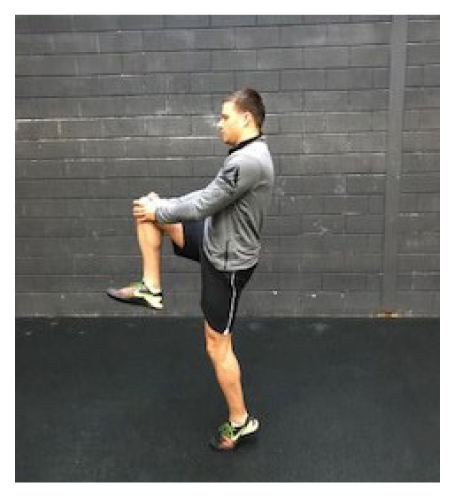
Jump, squat, push-up drill

Start in an athletic position. The coach calls out jump, squat or push up. Perform the exercise as indicated as fast as possible.
Shadow drill

Two cones are set up 10 yards (9 m) apart from one another. Two athletes stand facing each other in the centre of the cones. One athlete assumes the role of the leader. The other athlete must shadow the leader by mimicking his actions.