
Introduction
Periodontal diseases affect up to 90% of the global population and have become the most common oral health condition worldwide.1 Periodontitis, one of the well-known periodontal diseases, was estimated at around 62% and severe periodontitis at 23.6% among dentate adults between 2011 and 2020.2 Research on the correlation between periodontal disease and mental health problems, in this term as emotional conditions, has been developing since the 1950s.3 Research was initially limited to laboratories and animal testing, but has expanded to include humans, becoming an accepted tenet in the development of dentistry and psychiatry worldwide. This phenomenon has become an intersection of liaison services between the two fields (periodontics/dentistry and psychiatry), so it does not become a separate field of study.4
Several factors have been shown to mediate the putative relationship between biopsychosocial conditions and inflammatory periodontal diseases, such as stress-endocrine-periodontal changes,5 oral hygiene neglect,6 dietary intake changes,7 smoking and other harmful habits,8 gingival circulation,9 alteration in salivary flow and components,10 oral habits,11,12 host immune response1 and bruxism.13 Specifically, stress and its biochemical mediators may modify the immune response to microbial challenge, which is an important defence against inflammatory periodontal disease. When someone has a maladaptive response to a stressor, the release of adrenaline and noradrenaline may not only reduce blood flow but also decrease levels of essential blood components needed to maintain resistance to disease-related microbes. It may be that glucocorticoids, released during stress, prolong this vascular response.3
In someone with neurotic tendencies (anxiety, depression, acute stress reactions, panic disorder), it will direct their neurotic needs for oral expression due to their fixation in the psychodynamic phase at an earlier age.14 The mouth, as a source of gratification, becomes active, expressing feelings such as biting, sucking, tongue thrusting, thumb sucking, biting the tongue, lips, cheeks or fingernails.15 These actions also figure in bruxing, clenching, tooth doodling and smoking. Such habits may lead to tooth migration or loosening, as well as other periodontal problems. These neurotic tendencies can occur in anyone, including military personnel, who have the same chance of experiencing mental health issues and periodontitis problems that can appear simultaneously or superimposed.
Some factors that contribute to mental health issues and periodontitis in military personnel are the challenging work environment, extended deployments, limited access to healthcare during navigation trips, limited living space, monotonous daily routine, and disruption of the circadian rhythm and sleep–wake cycle, resulting in long-term oral health issues.16 There are direct and indirect explanations as pathomechanisms between periodontitis and mental health problems. However, many theories link them to the stress response, making them appear as superimposed cases that arise simultaneously. This issue requires attention to protect military personnel, the nation’s frontline security forces.
This research aims to provide an overview of the global condition of military personnel, specifically focusing on periodontitis cases superimposed with mental health problems among military personnel, which can later be interpreted as a description or sketch of the military situation. However, it requires interpretation based on each country’s background.
Material and methods
Protocol and search strategy
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines, available at http://www.prismastatement.org. Identification of pertinent studies was conducted through a comprehensive search of reputable databases, including PubMed, ScienceDirect, ResearchGate and Google Scholar. This review was conducted between June and August 2025, utilising a combination of the terms ‘periodontitis’, ‘mental health problems’ and ‘military personnel’. The identification of these keywords was achieved by combining synonymous terms and utilising advanced search techniques to enhance the understanding of existing material.
Inclusion and exclusion criteria
This review exclusively encompasses those that have been authored and published in the English language, adhering to specific inclusion criteria such as: 1) articles that were selected as observational studies (cohort, case control or cross-sectional), article reviews or case studies; 2) articles published in 2015–2025; 3) confirmed as periodontitis cases superimposed or overlap with mental health problems in military personnel. Exclusion criteria for selection were: 1) not an open-access article; 2) cases of periodontitis were never confirmed in military personnel; 3) article in commentary, supplementary, guideline, graphics, or data without analysis; 4) article not in English or Bahasa.
Data collection process
After searching for and collecting articles on the main topic, the main articles were selected by applying inclusion and exclusion criteria. They were then filtered with the CRAAP (currency, relevance, authority, accuracy and purpose) test. For the selection process, articles will be followed by information extracted from each article, including the author(s), year, country, research topics, study type, sample, data collection, analysis methods, and results. Differentiation of the military by region will introduce some divergence; therefore, this review will focus on an overview, a directional link, the causes, and a description of periodontitis cases superimposed on mental health problems in military personnel.
Results
At the first stage, 119 articles were identified, of which 60 remained after deduplication. Using predetermined inclusion and exclusion criteria and conducting feasibility tests with the CRAAP (currency, relevance, authority, accuracy and purpose) test, 50 articles were excluded. Finally, a total of 10 articles are to be included in the data synthesis (Figure 1). These articles were summarised in Table 1.
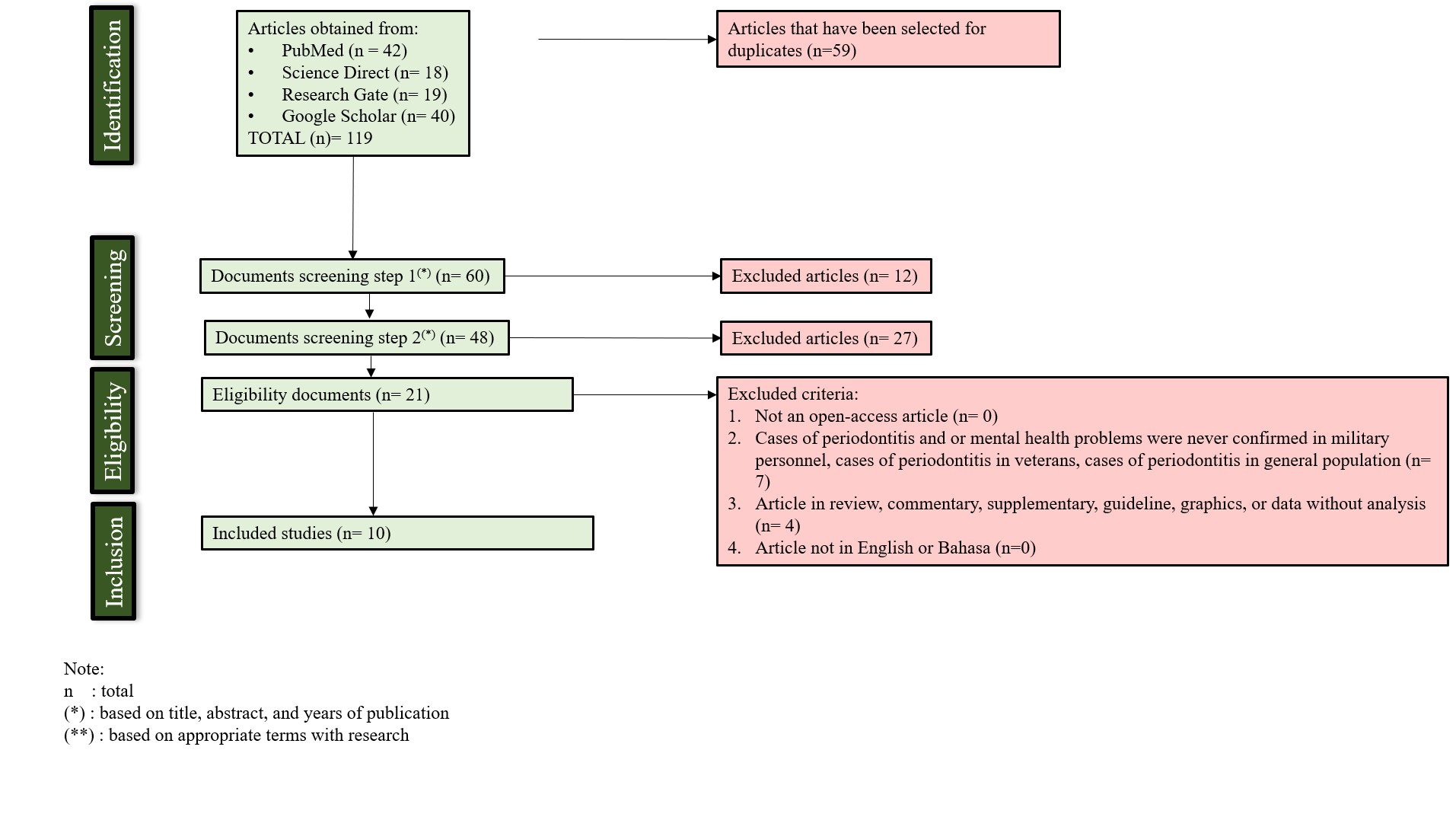
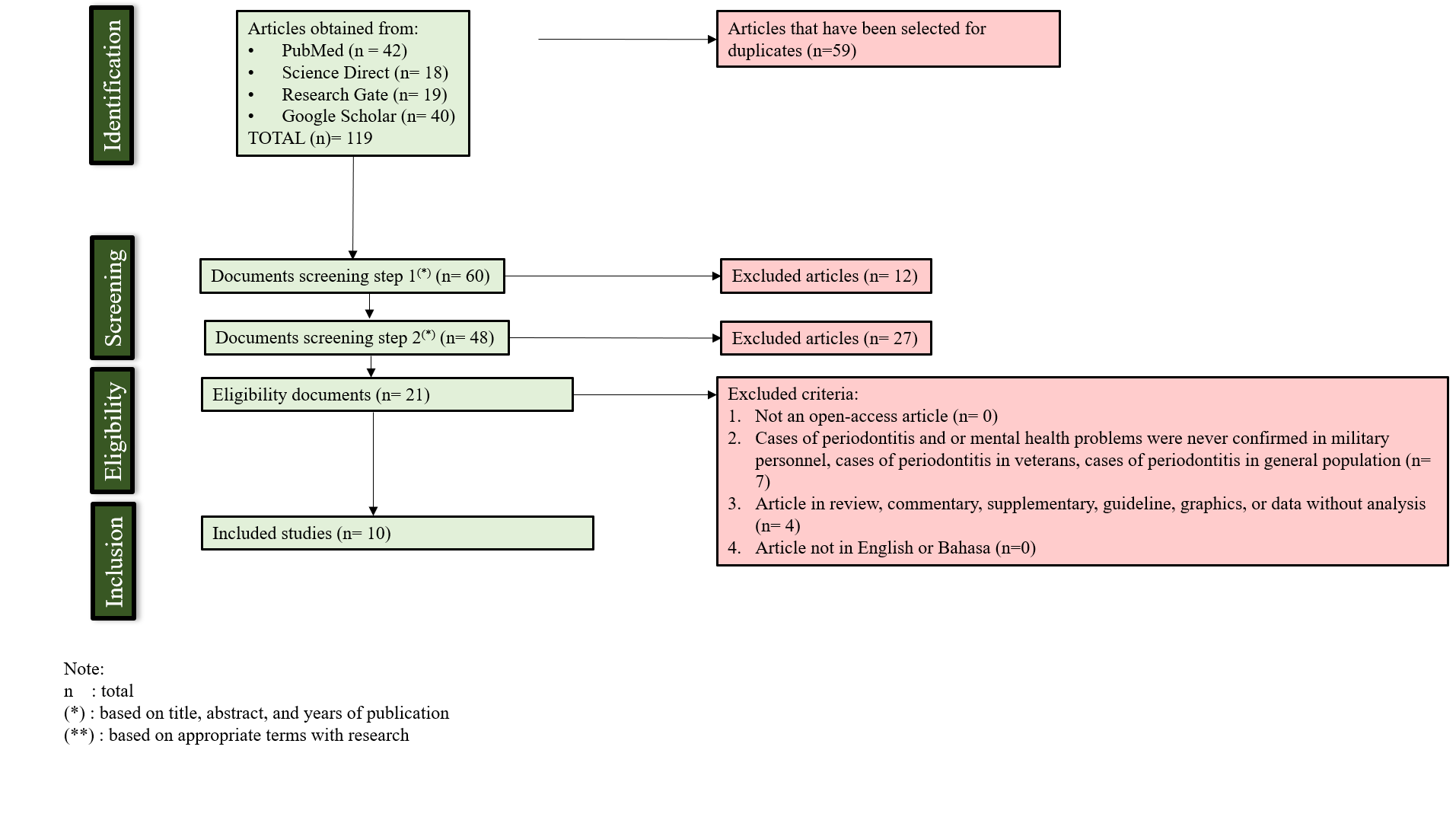
Figure 1. PRISMA diagram for literature selection
Table 1. Summary of key study characteristics
| Author(s) | Research topics | Type of study | Sample | Data collection and analysis method | Results |
| Solis, et al., 2017 [Brazil]17 | To investigate the impact of post-traumatic stress disorder (PTSD) on oral health. | case-control study | comprised 38 PTSD patients and 38 controls |
· Probing pocket depth (PPD), clinical attachment level (CAL), bleeding on probing and plaque were recorded at six sites per tooth. · A visual analogue scale (VAS) was used to evaluate the pain after probing. · The Research Diagnostic Criteria for Temporomandibular Disorders Axis II (RDC/TMD Axis II) and Structured Clinical Interview (DSM-IV) were also applied. |
· Patients with PTSD had a higher degree of chronic pain, more depression, and nonspecific physical symptoms (including and excluding pain) compared with the control group (Fisher’s exact test, p < 0.001, and Chi-squared test, p < 0.001, < 0.001, < 0.001, respectively). · Patients with PTSD also had more pain after periodontal probing compared with controls (Mann-Whitney, p = 0.037). · The prevalence of sites with CAL or PPD ≥ 4, ≥ 5, ≥ 6 were not different between the groups. · Age was associated with moderate periodontitis (multivariable logistic regression model, OR = 3.33, 95% CI = 1.03–10.75, p = 0.04). |
| Eger, et al., 2018 [Germany]18 | To analyse the relationship between periodontal disease and bruxism in soldiers with PTSD due to war stress, compared to soldiers without PTSD. | case-control study |
Total number of participants in the PTSD group: 123 (21 women, 102 men)
Control group: 36 male soldiers without PTSD, who also had a similar number of military assignments |
· 36 first-time hospitalised patients with psychiatric confirmed PTSD after up to 17 military foreign deployments, and 36, by age, number of deployments and number of teeth, matched male controls were included. · Dental examination included functional TMJ assessment, full-mouth periodontal status and jaw impressions for measurement of attrition. Necessary individual dental therapy is followed for every patient. |
Smoking was significantly positively correlated with chronic periodontitis in both groups (p < 0.05). Critical incident stress debriefing with bruxism and high mTWI is a hint at pathological stress susceptibility. Male soldiers with more than 2 years of PTSD suggest that excessive forces on dental occlusion are not likely to provoke any longstanding damage to the healthy periodontium, thus questioning the existence of pure primary trauma. |
| Eger, et al., 2021 [Germany]19 | To evaluate the relationship between dental anxiety and higher levels of SPS. | cross-sectional study | 116 soldiers, dental check-ups before deployment | referred with different stages of periodontitis for mandatory dental fitness before military deployment. | Dental anxiety showed moderately significant correlations with the SPS subscale Ease of Excitation (EOE), which measures emotional reactivity to physiological stimuli. |
| Worner, et al., 2021 [Germany]20 | To evaluate a possible relationship between bruxism and periodontal diagnosis. | cross-sectional study | 123 patients | Ninety-six in-patients and 27 outpatients (21 women, 102 men) with specialist-confirmed PTSD and bruxism after up to 17 foreign assignments, and 36 male non-PTSD controls with up to 15 foreign assignments underwent general dental, functional and periodontal examinations. |
· All three groups showed no statistically significant differences in age (34.8 ± 8.6 years), number of teeth (n: 26.3 ± 3.4), dental status (DMFT 9.7 ± 6.6), incidence of periodontitis (36%) and recessions (n: 5.8 ± 5.7). · From the control group to the outpatient group to the in-patient group, the proportion of smokers and tobacco use increased statistically significantly, as did the extent of attrition. · In the in-patient group, with statistically significantly lower educational levels, the number of perceived prophylaxis sessions was statistically significantly reduced over the last two years. |
| Tsai, et al. 2022 [Taiwan]21 | To examine the associations of decayed teeth and localised periodontitis with mental stress in young adults. | cross-sectional study | 334 military recruiters, aged 19–45 years, in Taiwan |
· Mental stress was assessed by the brief symptom rating scale-5 (BSRS-5), including five domains: anxiety, depression, hostility, interpersonal sensitivity, and insomnia (maximum score of 20). Those with symptomatic mental stress were defined as having BSRS-5 > 5 (n = 34). · Multiple linear and logistic regression models were used to determine the associations between decayed tooth numbers and periodontitis and BSRS-5, with adjustments for age, sex, education level, physical activity, body weight category and smoking status. |
· The BSRS-5 was positively correlated with decayed tooth numbers [β: 0.26 (95% confidence interval: 0.01–0.52)]. · Those who had more than two decayed teeth [odds ratio: 3.59 (1.52–8.46)] had a higher risk of symptomatic mental stress. · In contrast, the correlation between BSRS-5 and localised severe periodontitis was null. · Study recommended that decayed teeth, instead of localised periodontitis, was a risk factor for mental stress in young adults. |
| Kalaigian and Chaffee, 2023 [USA]22 | To examine mental health–oral health associations prospectively in a nationally representative US cohort. | cohort | Cross-sectional analysis (Wave 4): 30 746 adults (≥18 years old) Longitudinal analysis (Wave 5, after 2 years): 26 168 participants [based on inclusion criteria] |
· The Global Appraisal of Individual Needs–Short Screener measured three types of mental health symptoms: internalising, externalising and substance use problems. · Six self-reported oral health conditions related to periodontal disease were evaluated: self-rated oral health, bleeding gums, loose teeth, tooth extraction, gum disease and bone loss around teeth. · Cross-sectional analysis within PATH Study wave 4 (2016 to 2018, n = 30 746) compared the survey-weighted prevalence of the six oral health outcomes by severity of mental health problems. · Prospectively, oral health outcomes were assessed 2 years later (wave 5, 2018 to 2019) according to wave 4 (baseline) mental health problems (n = 26 168). |
· All six adverse oral health conditions were greater in prevalence among participants with severe internalising problems. Multiple conditions were also associated with severe externalising or substance use problems. Longitudinal associations attenuated, but multiple associations of meaningful magnitude persisted, most with internalising problems. Providers should expect higher levels of oral disease among patients with adverse mental health symptoms. Independent of externalising and substance use problems, symptoms of internalising problems (related to depression and/or anxiety) are plausible risk factors for future oral disease. · Better integration and coordination of mental and oral health treatment and prevention are recommended. |
| Bilan and Bandrivsky, 2024 [Ukraine]23 | To assess the periodontal tissue condition of military personnel in the Armed Forces of Ukraine based on their psycho-emotional state. | cross-sectional study | 142 male military personnel of the Armed Forces of Ukraine |
· The subjects’ age range was 27 to 60 years, and their time in the combat zone ranged from 3 months to 2 years. · The patients underwent clinical and dental examinations according to a standardised scheme, which included taking anamnesis and analysing patients’ complaints. The periodontal tissue condition was assessed using Danilevsky’s MF (1994) classification, with additions by Mashchenko IS (2002). · To identify symptoms of post-traumatic stress disorder (PTSD) in military personnel of the Armed Forces of Ukraine, the PSL-5 questionnaire developed by the National Centre for PTSD; determined the presence and degree of psycho-emotional stress in the study group using the methodology of Holmes TH and Rahe RH (1967); the level of reactive and personal anxiety was measured using the Spielberger-Hanin method, specifically the State-Trait Anxiety Inventory (STAI) from 1970. |
The study found a close relationship between the psycho-emotional disorders of the subjects and the condition of their periodontal tissues. This relationship is likely one of the leading factors that determine the intensity and severity of inflammatory and dystrophic-inflammatory diseases of periodontal tissues in this cohort of patients. |
| Palle, et al., 2024 [India]24 | To evaluate the occupational stress and periodontal status among Indian Army personnel. | cross-sectional study | 1000 army personnel divided into four groups of 250 each |
· Group A had recruits, Group B had trainee officers, Group C personnel were serving in the army below the officer’s rank, and Group D had officers who were currently serving in the army. · Oral Hygiene Index – Simplified (OHI-S), Gingival Bleeding Index (GBI), pocket depth, and clinical loss of attachment (CLOA) were assessed for periodontal status. · Stress levels were evaluated using the Modified Occupational Stress Index Questionnaire. · Analysis of variance (ANOVA) was used to compare OHI-S, GBI, pocket depth and occupational stress scores, while the Kruskal-Wallis test was used to compare the occupational stress index and CLOA among the study groups. |
The study revealed that the majority of army personnel were suffering from gingival bleeding and periodontal diseases; however, the association between stress level and periodontal diseases in Indian army personnel was less and not significant. |
| Setyawati, et al., 2025 [Indonesia]25 | To explore the oral and periodontal health of soldiers, with a focus on the relationship between stress levels and periodontal conditions in soldiers from Kodam Jaya. | cross-sectional study | A total of 48 male respondents were selected using a purposive sampling technique (soldiers from Kodam Jaya who were willing to participate and had periodontal tissue disorders) | All participants completed 10 closed-ended questionnaires about emotions and thoughts over the past month, along with the Perceived Stress Scale (PSS). Data processing was analysed using univariate and bivariate methods, including Spearman’s correlation. | The correlation between stress level and periodontal tissue health at BoP examination shows a moderate association (r = 0.407, p = 0.004), indicating a significant relationship. |
| Boitsaniuk, et al., 2025 [Ukraine]26 | To determine the relationship between stress and oral health in individuals exposed to chronic stress in wartime. | cross-sectional study | 68 professional soldiers Ukraine army, 42 internally displaced persons, control group of 39 persons | The study was based on clinical examination and a questionnaire. | Notable differences exist between the groups in wartime and peacetime, based on how often they brush their teeth daily and their diets. A group of soldiers had significantly poorer oral health than civilians. According to the plaque index, аmong the military, only 7.1% have good oral hygiene (plaque index 0.0), 53.6% have fair oral hygiene (plaque index 0.1–1.9), and 39.3% have bad oral hygiene (plaque index 2.0–3.0). |
Based on the scientific articles we summarised, it was evident that research in dentistry, psychiatry and the military has become a focus for professionals in each field. Several review papers were excluded, even though their knowledge bases were derived from field findings. Several secondary data sources, including narratives and literature reviews, reinforced theoretical elements and practical clinical applications in the field. A total of 10 articles that met the inclusion criteria showed that the direction of research is becoming increasingly complex, marked by a variety of mental health conditions such as PTSD, stress, anxiety, hostility, interpersonal sensitivity, insomnia, and substance use disorders. The correlation between mental health conditions in military personnel and dental health conditions, particularly periodontitis, is a global problem that can be found in various countries, such as Indonesia,25 India,24 Ukraine,23 the United States,22 Taiwan,21 Germany18–20 and Brazil.17
Several studies that met the inclusion criteria comprised two case-control studies, one cohort study, and seven cross-sectional studies, with the main focus of all studies being the evaluation of mental health and periodontal status in active soldiers. Examinations were conducted in several studies as part of routine screening for military personnel (soldiers) with status of dental clinic control patients or those undergoing treatment (inpatient care), and before deployment. Some similarities or consistencies in the results of these studies included epidemiological aspects, common aetiology, superimposed between two conditions (mental health problems and periodontitis), prognosis, and common direct suggestions (Table 2).
Table 2. Similarities in research findings
| Consistency of results | Description |
| Epidemiology |
· Periodontal disease is higher in soldiers with a history of PTSD than in controls (without PTSD).17,20 · Soldiers with a history of multiple cavities have higher stress levels.21 · Soldiers with high stress levels have greater periodontal severity (more attachment loss and pocket depth).24 |
| Common aetiology |
· Soldiers with low stress resistance and high reactive anxiety showed more severe periodontal damage [accompanied by higher gingival and periodontal indices]; on the contrary, soldiers with high stress resistance and low anxiety had better periodontal conditions.23 · Soldiers with high sensory processing sensitivity exhibit higher levels of anxiety and more severe periodontal disease and tend to be more anxious about undergoing dental treatment.19 · A two-way relationship was found: mental stress leads to poor oral hygiene, thereby increasing the likelihood of tooth decay and periodontitis. The emergence of these oral diseases will further increase the psychological burden on soldiers, thereby increasing the likelihood of stress. 21 · Biological mechanism linking stress and periodontal disease; behavioural factors mediating the stress-periodontal disease connection.25 · The influence of behavioural patterns [infrequent tooth brushing, skipping dental check-ups], lifestyle during war [malnutrition, limited access to health services, smoking habits, neglected oral hygiene] contributed to the destruction of soldiers’ periodontal tissue, accompanied by chronic stress that affected immunity and inflammatory responses in the body.22,26 |
| Superimposed between two conditions |
· Soldiers with a history of PTSD have a history of bruxism as one of the aetiologies of periodontitis,18 which, when localised periodontitis is found, will be positively correlated with mental stress scores.21 · Soldiers with a history of PTSD complain of more severe pain, especially after periodontal probing.17 · Depression and anxiety correlate with oral pain and poor oral health perception.22 · Soldiers with severe periodontitis tend to have higher dental anxiety scores.19 |
| Prognosis |
· Psychological factors such as stress and anxiety worsen the progression of periodontal disease in soldiers.23 · The emergence of PTSD and bruxism in soldiers is a strong risk factor for more severe periodontal damage.18 If bruxism tendencies accompanied by maladaptive coping behaviours persist over a long period of time, there is a risk of more severe tooth wear.20 · Soldiers with mental disorders and additional risk factors such as poor oral health, smoking habits and maladaptive coping stressors are prone to stress hormone dysregulation, which triggers poor oral health, risk of tooth loss, caries and periodontal symptoms.20,22 |
| Common direct suggestion |
· The importance of integrating mental health and dental health services into the public health system,22 as well as improving the quality of life and task readiness of soldiers, especially those with a history of PTSD or other mental disorders.20 · Special attention should be paid to psychological aspects and dental readiness in military health services,20 including soldiers serving in conflict areas or in military groups.26 · Stress management strategies and psychological interventions are needed. Good dental care interventions help reduce mental stress and prevent the progression of periodontal disease among young military personnel.21,23,24 |
Discussion
An interesting finding discovered during the filtering process using the PRISMA method was the large number of reports from various countries showing similar problems, such as Norway,9 Portugal,2,13 Saudi Arabia,12 Croatia,27 Turkey,11 Cameroon,28 Finland,29 Malaysia, 16,30 Iran,31 New Zealand,32 China,10,33,34 Italy,35 France,36 Canada,1 Spain,37,38 England,39 Belgium,40 Nigeria41 and Australia.42 This means that the problem of periodontitis superimposed with mental health problems is a concern for many practitioners and researchers in various countries. The intersection of these three fields (dentistry, psychiatry, and the military) is interesting due to the ever-changing global situation. Stress caused by the threat of war increases the likelihood of PTSD among soldiers, which not only weakens their psychological system but also their dental health. Similar stress is also experienced in countries not at war, due to the various factors soldiers face. The direct impact is the failure to achieve optimal health for soldiers, which poses risks to work performance, self-resilience, and even suboptimal dedication to the nation.
Veterans or retired soldiers are not included in the inclusion criteria, even though they have a military history. Veterans are no longer active in service, giving rise to the idea or assumption that their health condition is multimorbid with chronic stress typical of old age, or not accompanied by stress when they were still on duty. In the future, an in-depth study of veterans’ health profiles is needed, including a psychogeriatric assessment. However, we ultimately conclude that dental health and mental health can serve as a basis for diagnosis, therapy and prognosis for practitioners, given their overlapping interrelationships.
The findings of the above study led to several conclusions that the oral health and mental health of soldiers are dynamic and cannot always remain stable due to many factors. Based on the researchers’ observations, at least several factors or situations contribute to the occurrence of periodontitis, including: 1) Infrequent tooth brushing, resulting in plaque build up and the formation of tartar, which can cause gingivitis to develop into periodontitis; 2) Incorrect tooth brushing techniques, resulting in abrasion of the tooth surface; 3) The habit of chewing on one side because there may be cavities on the other side (which are not treated, allowing the lesions to develop), so that food deposits accumulate on the side that is not used for chewing, leading to the situation described in point 1; 4) Bad habits such as smoking, which cause micro vascularisation disorders in the capillaries in the tissue around the teeth and gums; 5) Bad habit of alcohol consumption; 6) Trauma to the oral cavity area; and 7) Systemic diseases suffered by the soldier that manifest in the oral cavity and vice versa.
In addition, researchers observed several factors contributing to the emergence of mental health problems among soldiers, including: 1) genetic factors; 2) stress factors and maladaptive responses to problems perceived as pressure; 3) personality factors; 4) responses to work situations and events beyond control; 5) failure or difficulty adapting to task assignments; 6) problems with endurance, flexibility, and vulnerability to differences in group dynamics; and 7) interpersonal and intrapersonal problems among soldiers. The phenomenon of global dynamics in oral and mental health among the military population may also occur in Indonesia. This leads to the idea of developing and protecting soldiers as the frontline of the nation’s security and stability.
The applied applications and implementation proposals submitted by researchers in the future, especially in Indonesia, are: First, from recruitment/acceptance of prospective soldiers, they are thoroughly selected in accordance with the health examination manual, where each examiner (military dentist) has been standardised (calibrated) periodically to minimise misinterpretation of the examination results. This can be realised by holding an Indonesian Army Dentist Perception Meeting every 6 months as a forum for communication, sharing, and networking among fellow dentists in the Indonesian Army environment (using a digital platform such as Zoom, Google Meet, or another video device, if the cost of official travel is too high). Second, have unit commanders conduct periodic health checks for soldiers to follow up on their dental and oral health at military health facilities. Third, support from the high command to equip the Indonesian Army with human resources and health facility infrastructure to support soldiers’ services.
Future research direction
This study is a systematic review with a scope of discussion on periodontitis superimposed with mental health among the military globally. This opens the opportunity to further explore the situation regarding physical, dental, and mental health among soldiers, especially in Indonesia, across the army, air force, and navy, to maintain optimal health and enable soldiers to serve the country effectively. Large-scale research in Indonesia will facilitate the mapping of health profiles and support strategic decision-making by leaders. In the future, research could develop in areas such as laboratory management or governance, screening, the use of tools, or genetics, which can trace a person’s vulnerability based on genetic polymorphisms.
Conclusion
Periodontitis cases superimposed with mental health problems among military personnel have become a global issue involving three fields: dentistry, psychiatry, and the military. These overlapping cases can serve as a basis for diagnosis, therapy, and prognosis, and should involve a comprehensive evaluation to minimise the long-term impact on soldiers.
Conflict of interest
The authors declare no conflict of interest.
Authors contributions
ZU: methodology, literature search, screening eligibility, data extraction, writing; SM: conceptualisation, methodology, screening eligibility, writing; BPS: quality assessment, supervision; RT: screening eligibility, data extraction, quality assessment; MLA: data extraction, data analysis; supervision; OSYW: data extraction, data analysis; supervision; KFE: quality assessment, supervision.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Please specify the URL of your file