
ABSTRACT
Nuclear, Biological and Chemical (NBC) Warfare remains as much a risk today as it has been in the past. With increased numbers of proliferating nations, increased industrialization and poorly effective arms control measures, this risk is unlikely to decrease in the foreseeable future. To prepare military physicians to deal with these toxic hazards, NBC medical training doctrine needs to be reviewed. Review of this doctrine has highlighted the need to enhance the current medical NBC training, both to align it with Emergency Management of Severe Trauma concepts and to target the most appropriate medical populations.
INTRODUCTION
At 1730 hours on 22 April 1915, the Germans released 150 tons to chlorine from gas cylinders against Allied lines at Ypres1. Modern chemical warfare had begun. This initial use was followed over the next four years by intensive use of chlorine, phosgene, sulphur mustard and other chemical agents by both sides. Casualties number 1.3 million, including 91,000 deaths, were attributed to chemical warfare2. Subsequent chemical agent use was to occur in scattered conflicts over the next 75 years, including the Italo-Abyssinian War, the Sino Japanese War and the recent Iran-Iraq War3. Nerve agents were discovered by German scientists in 1936. Fortunately, no chemical agents were used in the Second World War4. The continued danger of chemically induced injury to both military and civilian personnel has been illustrated by a number of catastrophic industrial accidents, including Bhopal where 2,500 people died following an industrial methyl isocyanate leak in 1984.
Biological warfare has been with us for millenniums. From the dropping of cadavers into wells to the throwing of plague victims over the walls of Caffa,6.7 biological warfare has existed in one form or another. Modern biological warfare began in a laboratory in Pingfan, Manchuria in 1936 where biological warfare agents were methodically studied, experimented with and ultimately used by the Japanese against the Chinese in the Sino-Japanese war8. Although no further validated use has occurred, there have been numerous allegations of use of both biological and toxin agents in various conflicts, including the Korean and Vietnam Wars.
The nuclear warfare age was initiated with the explosion of an atomic device over Hiroshima on August 6, 19459. This 12-kiloton weapon produced 45,000 deaths and 90,000 casualties in the 24 hours. 10 A second device was dropped on Nagasaki on August 8, 1945. In 1949, the Soviet Union tested their first nuclear weapon. The nuclear arms race had begun. By 1983, at the height of the Cold War, the United States was estimated to have 9,719 nuclear warheads, the Soviet Union,
Nuclear, Biological and Chemical (NBC) warfare has been with us as a major military risk for over fifty years. Research into NBC medical countermeasures, agent detection and protective equipment has progressed slowly over this period. Successes have included the development of effective nerve agent treatment protocols, chemical warfare agent detectors and individual protective equipment.
RISKS
The necessity for continued resourcing, in both monetary and personnel terms, of medical NBC doctrine, research and training, remains. The risk has changed with the demise of the Soviet Union but has not disappeared. In 1993, more then 24 countries are confirmed or suspected of having an offensive chemical warfare programme. Fourteen countries have or are suspected of having an offensive biological warfare programme and sixteen countries have confirmed or suspected nuclear weapons programmes. A number of countries have programmes in two or more of these areas. This represents a marked increase in the number of countries with offensive NBC programmes since 198012. Notably, Russia has continued research into offensive biological warfare agents despite strong United States and British diplomatic pressure, and trilateral inspections. 13 in addition, as the Gulf War has illustrated, Allied forces continue to be threatened by NBC weapons in certain operational scenarios.14 These weapons will continue to pose a threat to Australian forces in future deployments regardless of the region or the level of conflict.
This growth in NBC capability is despite the Geneva Protocol of 1925, the Nuclear Non-Proliferation Treaty of 1986 and the Biological Weapons Convention of 1972. The latter two treaties have suffered because they have not included key participants, have not called for gradual disarmament and, in the case of the Biological Weapons Convention, have not had adequate verification procedures. Periodic review conferences have endeavored to bolster confidence in the Biological Weapons Convention by increased openness and communication between participants15, but the success of such measures remains uncertain.
The new Chemical Weapons Convention should address these concerns in the chemical and toxin agent area. The Convention will not come into force until 65 countries have formally ratified and, if the ratification times of previous treaties are indicative, ratification may take years. Even then, continued problems are expected with the verification procedures.
There are related problems. Increased industrialization is occurring in many parts of the world. In particular, many countries have large chemical industries which use chemicals like chlorine, phosgene, cyanide and isocyanates, in their processes. 15.17 The risk of accidents from these industries is not negligible. The nuclear industry has also expanded with the building of many new reactors over the last twenty years. Some, like the ill-fated Chernobyl reactions and the Ignalina reaction in Lithuania, have inherent design problems18. Conflicts are now developing in areas where there are established chemical, nuclear medicine and even biological research facilities (e.g., Former Republic of Yugoslavia). Accidental or malicious release of agents from one these facilities is certainly feasible and the toxic gas leak at the Union Carbide plant in Bhopal,19 the nuclear reaction accident at Chernobyl, the explosions at the plutonium production facility at Chelyabinsk /0 and the accidental release of anthrax from a biological weapons research facility in Sverdlovsk in 1971, 21 all illustrate the dangers of such release.
MEDICAL NBC TRAINING
NBC Defence medicine is an area of medicine that is both highly specialised and not routinely considered or taught in a medical setting. Medical expertise in this area is limited in the military and is practically non-existent in the civilian area. This deficiency needs to be addressed at a number of different levels. In the military setting, there needs to be training at the paramedic, first-line medical officer, nursing officer and medical service officer level. As low-level situations, such as peace-keeping in Rwanda or Somalia, may require the rapid deployment of medical assets, medical personnel need medical NBC training in advance.
To achieve appropriate NBC medical support, medical personnel can either be trained to an appropriate NBC specialist level or be given basic training and supported with specialist teams. The extensive training of all personnel, whilst desirable, is neither practical nor realistic. This training would require in-depth instruction in intensive care procedures and in all facets of NBC defence. This would involve long periods of instruction, attachments to both intensive care and NBC units, and frequents refresher courses. This would be expensive, both in time and money, and is unlikely to be effective due to the high degree of skill fade that occurs when this expertise is not put to constant use.
The basic training of medical personnel with specialist team support is the preferred option. All medical personnel should be trained to a basic NBC resuscitation level in order to keep the casualty alive until either the patient is medically evacuated to third line care or the unit can be reinforced with medical specialists. Additionally, there is a requirement to identify teams with specialist NBC knowledge who can provide support and advice to medical commanders at short notice. These teams would come primarily from the Aeronautical and Maritime Research Laboratory (AMRL) and the Office of the SGADF.
This training should fulfil a number of criteria.
Firstly, it should be tri-service and should utilise tri-service resources. The principles of treatment are applicable to all three services and this course would complement the general single service NBC courses. It would also form a good foundation from which the student could progress onto other more advanced courses like the Medical Officers NBC Course and the Defence Radiation Protection Officers Course.
Secondly, the training should be based on the basic resuscitative principles outlined in the Emergency Management of Severe Trauma concept. These concepts, once developed, can be applied to other industrial toxicological emergencies and could be usefully applied in the medical training of civilian health personnel.
Thirdly, the training should initially be directed at all junior medical and health service officers who may be required to put these concepts into action. Courses for paramedics and other health service personnel would be developed to teach these principles whilst incorporating their specialist roles. Medical specialists providing third and fourth line care would also receive an appropriately directed course to enable them to carry out their function. These specialists will form the Reserve nucleus from which a coherent response can be developed by the Departments of Health. Revision courses every three years would ensure that the medical personnel would remain current.
Finally, the training should provide the treatment protocols and handbooks to support the medical person in the field and should be overseen by an appropriately trained medical adviser.
The most effective way of training health service personnel is to tie the NBC training in with current training. Emergency Management of Severe Trauma (EMST) course are already part of the general training of all ADF medical officers. Whilst extremely useful in what they achieve, the EMST courses have some disadvantage in the military context. Firstly, they are targeted at civilian trauma primarily and not a Combat Casualty Care. Secondly, they are principally designed for medical officers and not other health service personnel. The United States Army runs Combat Casualty Care course incorporating EMST but still provide minimal trauma management training, military or otherwise, to their corpsman. 23 The Royal Army runs both battle orientated EMST courses (Battlefield Advanced Trauma Life Support – (BATLS) and EMST courses for military paramedics and other health service personnel. These concepts are being considered in the development of an Australian Combat Casualty Care course.
EMST principles can be applied to not only to trauma and bums but also to the medical management of NBC casualties. To implement these concepts a BATLS (NBC) course is being jointly developed between the United Kingdom and Australia. The BATLS (NBC) course would be a short course designed to give the basics of the medical management of NBC to students. It would be divided into 3 modules.
| Module 1 | Introductory lectures covering NBC risks, concepts of NBC defence and medical NBC doctrine |
| Module 2 | Symptomatology, diagnostic algorithms and treatment protocols. |
| Module 3 | Scenario based exercises for each of the NBC subjects. This phase will include short briefs on intelligence, delivery systems, hazards and the specifies of management of NBC casualties. |
This structuring will allow one or more of the modules to be exported. The modular system can be adapted to the different groups needs. Module 2 alone will fulfil many of the requirements for paramedic training whilst Module 3 may be adapted to the specialist requirements of nursing officers, dental officers, medical administration officers and specialist medical officers. As well as developing basic knowledge across the ADF, this system could be easily incorporated in current courses (Health Service Officers’ Acquaint Course, Phase 4 Training) and would be useful preparation for the Medical Officers NBC Course, which would provide the greater depth of knowledge and medical planning skills required to manage multiple casualties in an NBC environment.
Figure 1 illustrates this concept as it applies to the management of nuclear, biological and chemical casualties respectively. Additionally, as industrial toxicological problems are of growing concern to both the military and civilian medical communities, these concepts will be presented to the Royal Colleges for incorporation in their training programmes.
CONCLUSION
Nuclear, biological and chemical warfare remains a military threat as we near the end of the twentieth century. Military medical personnel must be trained to deal with this threat and should be trained in such a way that the resuscitative principles learned will be applicable to toxicological emergencies beyond those of NBC warfare. Appropriate medical NBC training and the constant review of the NBC medical doctrine, policy and counter-measures, will ensure that the military medical personnel are ready for any military contingency, large or small.
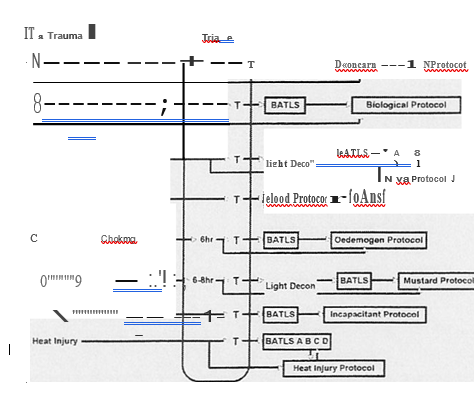
Figure 1: BATLS (NBC)