
Abstract
Although Special Forces may expect high casualty rates, such highly-trained soldiers cannot afford infectious disease losses. During World War II, malaria often determined the extent of special operations simply by limiting the time a unit could be deployed in a tropical jungle before fever incapacitated it. During the Allied campaign against the Imperial Japanese Army in Burma in 1943–1944, long-range penetration patrols by both the United States (US) Army (Merrill’s Marauders) and British/Indian Army (Chindits) were heavily affected by malaria, causing the majority of their disease casualties. In the Australian Imperial Force, 2/2 Independent Company were eventually evacuated in late 1942 after months in East Timor with essentially all survivors infected with malaria. Chemoprophylaxis remains the best preventive intervention to keep heavily exposed soldiers free of malaria symptoms. Improved regimens that are better tolerated and last for extended periods are still required.
Special Forces operations are often of such short duration that infectious disease incubation periods minimise mission impact. This is not true for long- range penetration patrols that may last for weeks, such as in Burma and East Timor during World War II. In several cases, malaria and other infections such as scrub typhus and dysentery largely determined the interval before the infantry became combat ineffective. In the Indo-Pacific region, rugged jungle terrain remains the site of ongoing guerrilla warfare and is often where conventional military units cannot be usefully deployed. Special Forces units designed to move lightly across challenging geography may be considered in such situations. However, planners need to have realistic expectations about what even very fit and highly-trained military specialists can do under such circumstances. The historical records of Merrill’s Marauders (US Army) and the Chindits (British/Indian Army) in Burma 1943–1944, as well as the Australian Imperial Forces 2/2 Independent Company in East Timor in 1942, are briefly reviewed in regards to their malaria experience. Malaria was a devastating illness for all three units and severely compromised their combat effectiveness. Malaria remains a current threat in many parts of the Indo- Pacific. Better medical countermeasures are still needed to maintain Special Forces as a military option in the region.
Merrill’s Marauders in Burma
‘Concomitant with increasing fatigue, [and] acquirement of other diseases, such as the dysenteries, morale began to deteriorate and malaria discipline suffered greatly. No attention was paid either to clothing, repellent, or the use of atabrine. As this process went on, the impression of the medical officers was that a large number of men deliberately exposed themselves or at least welcomed the incurrence of malaria infection.’ MAJ Maurice Seltzer (1944).1
Merrill’s Marauders (Composite Unit 5307, later 75th Rangers) was the only combat infantry unit deployed in the China-Burma-India (CBI) theatre by the US Army during World War II.2 The military intent was to spearhead a north-to-south offensive of large bodies of US equipped Chinese Nationalist Army soldiers to clear the tenuous logistical link from Indian ports into southern China over the mountains of northern Burma3 (see Figure 1). In a series of three jungle operations by 3000 infantry soldiers supported by their Chinese and Kachin allies but supplied only by variable airdrops from February to July 1944, an entire Imperial Japanese Army division was largely neutralised, and the key Myitkyina airfield was captured. However, Merrill’s Marauders then disintegrated as a formed unit from tropical disease casualties and starvation and was never reconstituted following the prolonged siege of Myitkyina. Controversy still exists about the unit’s unconventional mission, high casualty rate and widely-perceived inadequate recognition for its accomplishments.3

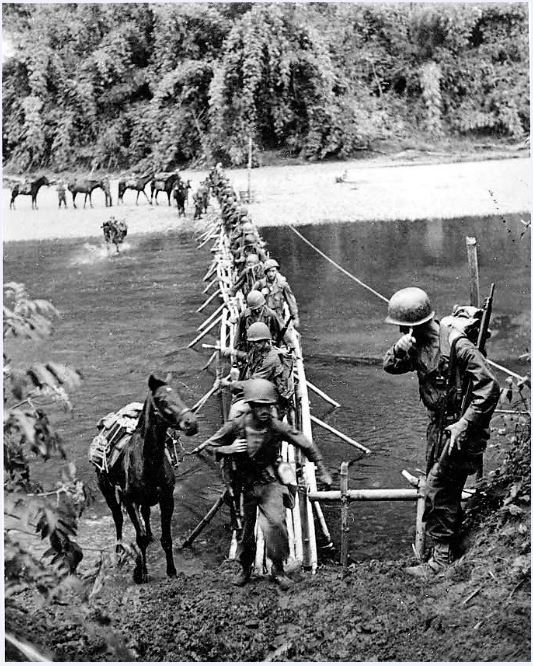
Figure 1: US Infantry Regiment (Provisional Unit 5307, later 75th Rangers) known as Merrill’s Marauders crossing a stream in the Kumon Mountains of northern Burma in March 1944. US Army official photo, now in public domain
Even in retrospect, it is difficult to give a complete account of Merrill’s Marauders malaria experience. However, it was unquestionably high and severely affected combat effectiveness.1 Malaria was a problem for Merrill’s Marauders even before starting their mission because nearly one-third of its members were veterans from the Solomon Islands campaign who were already infected with malaria. During the training phase, 7.4% per week of the soldiers became malaria casualties in India due to previous infections — removing men as unfit for duty with a history of three successive malaria attacks would have largely eliminated one of three infantry battalions if that proposed policy had been enforced.1 Few deaths resulted from malaria (unlike scrub typhus in the pre-antibiotic era). However, nearly all 5307th Unit’s members contracted malaria in Burma, of which 296 (10%) are listed as having been evacuated primarily for malaria. Another 950 men were evacuated as ill, for which most, if not all, had some malarial component. The bar for malaria evacuation was high, requiring a fever exceeding 102°F for three successive days despite quinine treatment.3 Variably drug- suppressed (usually with atabrine, aka mepacrine) malaria in Merrill’s Marauders was more typical of prisoners of war along the Thai–Burma Railway than in other Allied units as there was no medical policy enforcing regular atabrine suppression in CBI until August 1944, long after its worth was recognised on Guadalcanal and New Guinea. 4,5 CBI’s theatre-wide malaria rate fell from 320/1000 men to 20 over the course of one year, largely reflecting the disciplined use of the unpopular but effective mepacrine daily chemoprophylaxis. 4,6 It turned men’s skin yellow and was reputed to cause many other adverse events; however, it also unquestionably prevented malaria and was a decisive difference between the Allies and the Japanese whose medical supply system had collapsed.
Chindits in Burma
‘Statistically considered, Special Force met a more dangerous enemy in disease than in the Japanese Army. Clinically analysed, it was more severely injured by malaria and dysentery than by bullets and grenades. Tactically appraised, its battle worthiness was determined by its medical discipline more than by its courage.’ COL (later MAJGEN) W J Officer RAMC (1946) 7
The birth of modern British Special Operations includes the World War II experience of the Chindits, who evolved into a long-range, light infantry force sent in multiple small columns behind enemy lines in Burma to disrupt Japanese supply lines in coordination with an offensive by conventional forces. The first Chindit force (Operation Longcloth) in February to April 1943 was most remarkable for its casualties as nearly one-third of the force did not make it back across the Irrawaddy River to India (2182/3000 survived, 600 of which were unfit for any further service; see Figure 2). Those too ill to continue were ordered to be left behind with no hope of air evacuation and the predictable adverse effects on unit morale and cohesion. The second Chindit force (Operation Thursday, February to August 1944) formed an entire infantry division (20 000 men, nominally the 3rd Indian Division) and was better supported by air supply and some medical evacuation. The casualties were again high (1396 killed, 2434 wounded, half of the survivors were hospitalised).7 The success of the Chindit Operations was clearly qualified and has since been debated, especially in regards to how much or little it diverted enemy forces from their main effort against Assam in India.6,8,9
Because of multiple causes of infection in the tropics, it is difficult to evaluate how much of the immense

tropical disease problems experienced by the Chindits was explicitly due to malaria. LTCOL John Masters, a staff officer and temporary commander of the Chindit 111 Brigade in Burma, was well aware that some malaria breakthroughs resulted from the deliberate failure of men to take atabrine regularly. Casualties of 111 Brigade at the beginning of June 1944 (82 dead, 206 wounded, 49 missing) were nearly matched by those evacuated with disease (318), much of which was due to malaria. Although poor chemoprophylaxis discipline contributed to the malaria epidemic, in Master’s opinion, the rapid rise of sickness in the summer of 1944 among the Chindits resulted from their general debility, which had accumulated during an excessively long campaign (beyond the initial 90 days planned).7,8 In a medical review of 111 Brigade (nominal strength of 4000 soldiers) one month later, during July 1944, it was found that 4.3% had been killed, 9.8% were wounded, 46.5% were sick or wounded — enough to require evacuation — and only 4.4% (about one company equivalent) were functional. Malaria formed 61% of 111 Brigade’s medical casualties, and its illness rates were higher than any other unit. West African soldiers in the Chindits had half the malaria casualties seen in 111 Brigade. However, this was also true of the Gurkhas from Nepal, suggesting that this diminution was due to better chemoprophylaxis discipline among the tribal soldiers and not genetic/ immune resistance.
Regardless of its genesis, the mid-1944 malaria epidemic in the Chindits was a major limitation on human resources and thus combat effectiveness (see Figure 3). Based on a medical survey by the Deputy Director of Medical Services that the Theatre Commander ordered in July 1944 to determine if operations could continue in the face of such disease, it was estimated that most men had lost 28–42 pounds of body weight, most had been treated for malaria seven (minimum three) times while behind enemy lines and only about one-quarter were capable of any useful military effort. From three brigades nominally of 11 200 soldiers, 1300 were killed, wounded or missing, 7500 were sick enough to require medical evacuation and only 3400 could be listed as fit for duty. Just as Merrill’s Marauders had collapsed from cumulative disease casualties driven by malaria, the Chindits followed the same trajectory shortly thereafter in Burma.7
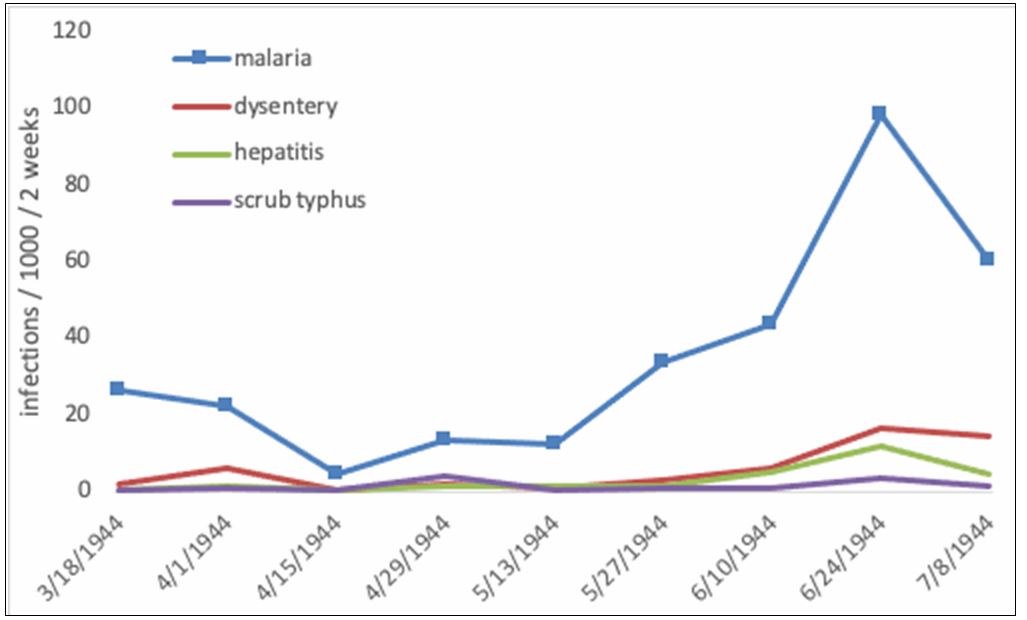
Figure 3: Chart showing medical casualty rates per 1000 soldiers by infection (malaria, dysentery/ diarrhea, hepatitis, scrub typhus) in Chindit Special Force March to August 1944 by fortnight. From Deputy Director Medical Services report.7
Australian Army in East Timor
‘As the men went down like flies with malaria, Dunkley begged and borrowed to treat his sick patients and began investigating what could be done to stem the spread of the illness. Dunkley’s recommendation to move the entire unit to the mountains west of Dili saved the company from certain capture.’10
Three Australian Imperial Force infantry battalions were placed as sentries in the outer island defence of Australia in 1941 in New Britain, Ambon and East Timor. All collapsed quickly in the face of the Imperial Japanese Army’s centripetal offence of early 1942. The malaria history of the survivors from Rabaul, New Britain, was horrific, with those falling behind due to malaria being massacred at the Tol Plantation.5 In East Timor, many of the soldiers of the 2/2 Independent Company were able to retreat from the Dili airfield into the surrounding hills and conduct a guerrilla campaign throughout 1942 with the help of local East Timorese allies10 (see Figure 4). So surprising was this that Australian radiomen in Darwin were sceptical of the force’s actual existence when a signaller on East Timor in April 1942, finally able to repair a small radio, sent out a statement of the company’s survival with an urgent request for boots, quinine, money and ammunition, given in that order of priority.10 Supplying the cut off soldiers by ship from Darwin was hazardous due to Japanese air attacks and resulted in the loss of HMAS Armidale. The small band of Australian soldiers with its East Timorese allies fought on for several months. However, increasing antiguerrilla activities of the Imperial Japanese Army and its retaliation against civilians necessitated the eventual evacuation of the sick and starved company survivors at the end of 1942.
Malaria had caused many casualties among the 2/2 Independent Company in East Timor. The first two platoons arrived in Dili in mid-December 1941. By early January 1942, it was estimated that 80% had malaria requiring the medical officer, CAPT Roger Dunkley, to set up a make-shift hospital housing for up to 80 patients, which had to be moved frequently to avoid the enemy.10 Relapsing malaria became a recurring theme as there were insufficient antimalarials to do anything other than suppress the acute attacks as they occurred at nearly monthly intervals. It is estimated that 40 of the 248 men of the 2/2 Independent Company were killed on East Timor in combat/accidents; however, none died of malaria, despite nearly all having been infected.

Figure 4: 2/2 Independent Company of the Australian Imperial Force in East Timor in 1942 showing burning houses with local fighters armed with spears. Australian War Memorial photo AWM 127992, now in the public domain.
Small special operations missions usually last only a few days prior to rapid exfiltration and recovery, placing little emphasis on infectious diseases with several days’ incubation period. However, the historical record of World War II suggests that when larger bodies of troops are sent behind enemy lines, such as Merrill’s Marauders and the Chindits in Burma, their health and combat performance can be degraded rapidly by indigenous tropical diseases such as malaria. Casualties, especially when they cannot be evacuated, become much more than a medical or logistical difficulty — sick and particularly dying comrades place an enormous strain on unit morale and cohesion when it is most critically needed. Bypassed units that converted to guerrilla warfare, such as the 2/2 Independent Company in East Timor, slowly starved when cut off from food supplies and sickened when deprived of malaria medications. Great Power competition is a current political reality across the island nations of the Indo-Pacific Region, and comfortable assumptions about future wars may no longer hold true. Special Operations often are confronted by great challenges and have to succeed by innovative means rather than brute force. Studying previous tropical campaigns can guide the anticipation of medical scenarios beyond those garrison forces face. Many such campaigns were determined by tropical infectious diseases such as malaria, arguing for continued development of improved medical countermeasures against such natural biological threats, particularly for those Special Forces units deployed into geographically difficult areas.
Corresponding Author: G. Dennis Shanks, Dennis.Shanks@defence.gov.au
Authors: G. D Shanks1,2
Author Affiliations:
1 ADF Malaria and Infectious Disease Institute
2 University of Queensland – School of Public Health Herston



