
Abstract
Black measles (Rubeola nigra) was understood to be an infrequent, severe subtype of measles defined by a very dark, nearly confluent rash in the 19th century. During the US Civil War (1861–65), measles epidemics killed many military recruits on both sides, with a case-fatality rate of 2%. Medical officers described black measles as appearing in the second week of illness and often leading to death. Black measles disappeared by the 20th century, and what clinical entity existed during the US Civil War is unclear. If one dismisses a faulty clinical diagnosis, the most likely explanation is a defect in cellular immunity due to nutritional deficiency or epidemiological isolation. Measles infections of rhesus monkeys show severe rash when CD8+ lymphocytes are suppressed. Rather than a historical footnote, black measles could be seen as a severe aspect of measles infection in an immunocompromised host.
Key words: measles, US Civil War, historical epidemiology, immunocompromise, military
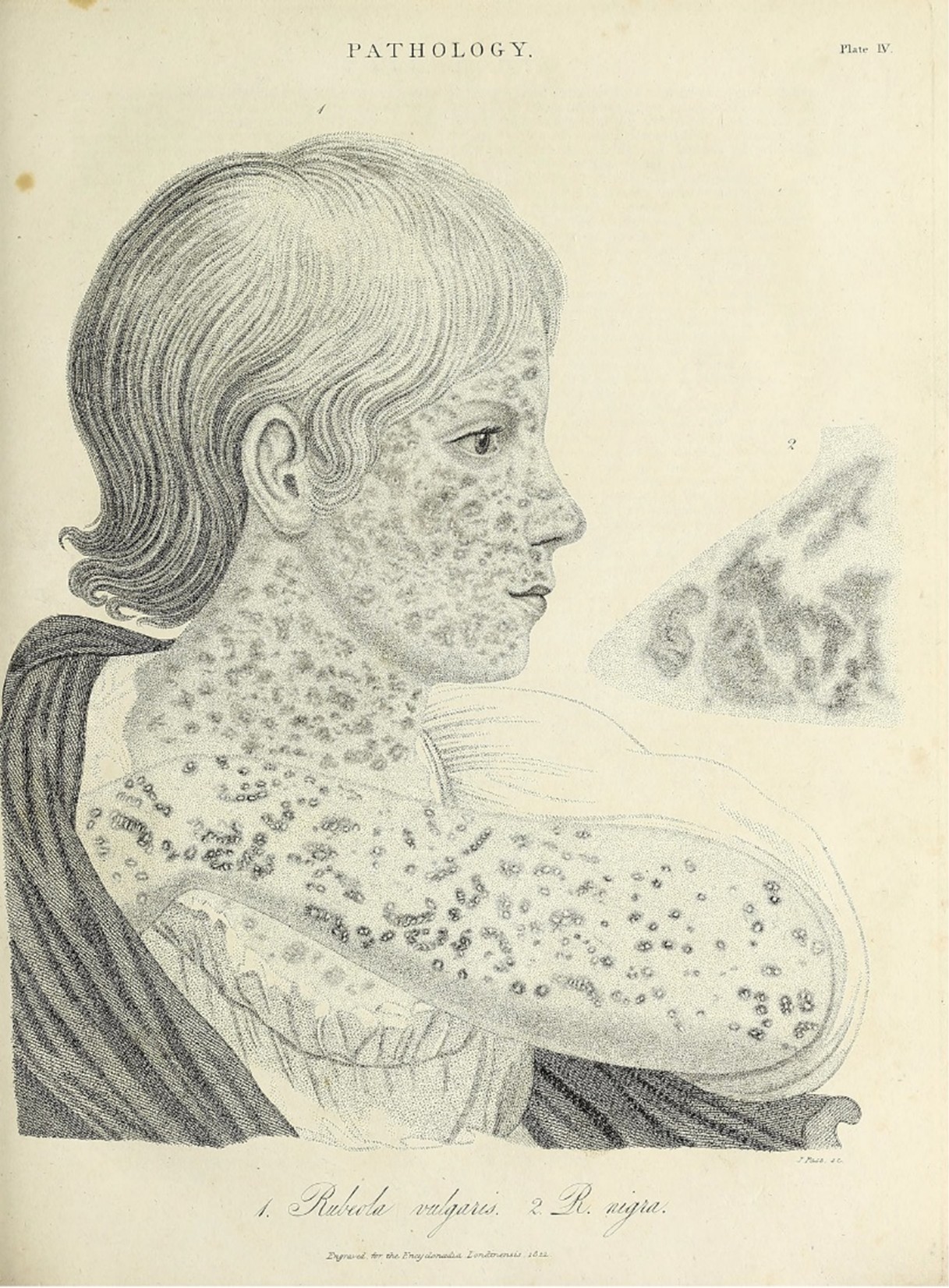
In the most dynamic cases the eruption is of a livid, reddish or blackish purple, scarcely modified by the pressure of the fingers. This is the variety which has been described as rubeola nigra, or black measles, and is particularly fatal.1 MAJ Joseph J. Woodward 1863
A majority of soldiers who perished during the US Civil War died from disease, primarily infections such as dysentery, typhoid, malaria and measles.2 Measles was a particular problem in newly recruited soldiers as they often came from isolated farming communities and had not previously been exposed to this highly infectious respiratory pathogen. ‘Camp measles’ was so common that some commanders did not want to receive newly formed regiments until they had undergone the ‘seasoning’ as an almost inevitable rite of passage into the 19th-century military system.1 Measles carried a substantial mortality rate or tax on recruits of about 2%, and some cases of particularly severe measles were labelled as black measles due to an almost haemorrhagic rash. It is uncertain what this clinical entity might be as there have been no reports of black measles in the 20th century. The historical records of the US Civil War have been examined in the light of modern pathology and immunology to suggest what our scientific predecessors might have designated black measles in the 19th century.
Woodward’s description of black measles appears at the beginning of this article and is the most detailed, as most refer only to the great lethality of black measles. Outbreaks of measles often occurred before soldiers formally entered the military system, limiting published observations other than those scattered in soldiers’ letters to family members. One epidemic that at least is said to have included black measles was reported in the Confederate Army in Camp Beauregard, Kentucky, during the winter of 1861, but the very high mortality list (up to 1500 out of 6000 soldiers overall, including measles) indicates that multiple pathogens were involved in this disease disaster. After 4 months the camp was evacuated and burned by its commander as a sanitary measure.3 As the war progressed, there were fewer camp measles epidemics as the flow of recruits slowed with waning enthusiasm for what had become a grim war of attrition.4 Measles killed many, including nearly 5000 Union soldiers, but so did other diseases, particularly of the gastrointestinal tract and black measles was largely forgotten as an extreme example of a recruit camp disease.2 Medical officers of the US Civil War were handicapped by many pre-modern concepts of disease causation (e.g., miasmas), but were very competent clinical observers. Although it is possible that black measles was diagnostically confused with other severe infections such as haemorrhagic smallpox or meningococcal disease, neither of these was common either. It seems unlikely that a severe manifestation of measles was routinely misclassified if only because nearly all 19th-century physicians were very familiar with measles, and black measles was usually stated to be a later manifestation of the disease. An alternative view is that ‘black’ was an adjective applied to any severe infectious disease along the lines of the ‘black death’ and was only a designation of its serious, lethal nature.5
The historical understanding of rubeola nigra can be partially reconstructed from the pre-Civil War literature. A classical set of lectures on diseases of the skin from The Lancet list four types of measles, of which rubeola nigra was the least common and most severe.6 Repeating a previous authority, Rayer, in the 1842 lecture for medical students, black measles occurs in the second week of illness when the rash markedly darkens to deep purple, spreads beyond the pre-existing measles rash to become nearly confluent and is often associated with a bleeding phenomenon such as petechiae and ecchymoses. One of the few illustrations of this phenomenon comes from a British encyclopedia of 1823 (Figure 1) and has an inset said to contrast the rash of rubeola nigra with its common version (vulgaris). Other than being irregular and more confluent than rubeola vulgaris, it is hard to gather more from the figure than already stated in the text.7
Severe measles in military populations certainly existed into the 20th century, but it was primarily due to the recruit soldiers’ susceptibility to secondary pneumonia following measles especially due to Streptococcus pyogenes.8 Mortality and severe sequelae such as pulmonary abscesses resulted when measles patients were crowded into World War I hospitals in the pre-antibiotic era. Secondary bacterial pneumonia after measles was confided mainly to the winter in less crowded circumstances without generalised military mobilisation, indicating the importance of crowding on colonisation by bacterial pathogens causing secondary pneumonia.9 Measles mortality progressively fell in the US Army over time as increasing population mobility increased childhood measles incidence and made adult measles an increasingly unusual event in the USA.10 Despite the severity of measles in the US Army during World War I, there were no descriptions of black measles in the Official Medical History as during the Civil War.11
Measles is severe and often lethal in immunocompromised persons, including primary deficits such as children with congenital cellular immune defects and secondary immunocompromise due to protein-calorie malnutrition. Congenital immunodeficiencies and measles seem to be dichotomous because children with only humoral defects (e.g. agammaglobulinemia) manage measles infection relatively well, while those with cellular defects do very poorly.12 Measles mortality is particularly severe in African refugee children suffering from malnutrition, and sometimes, the rash deepens to a deep red or purple colour. The type of measles rash in malnourished African children has suggested that black measles is actually measles in an immunocompromised person. However, it is not routinely designated as black measles, perhaps because of their darker skin colour.13 Experimental measles infections in rhesus monkeys have been instrumental in working out the pathogenesis of the measles rash.14 The measles rash occurs when lymphocytes and other immune cells interact with virally infected cells in the skin, usually two weeks after exposure to the virus. Children with little cellular immunity often have no rash during a severe measles infection.15 Experimental infections in rhesus monkeys whose CD8+ lymphocytes have been depleted have severe measles rash, suggesting that an immune imbalance is the cause of phenomena such as black measles.16
Another aspect that may have played a role in the disappearance of black measles in modern times is severe measles in epidemiological isolated groups such as on Pacific Islands when measles first arrives in a non-immune population. One of the last such examples was the 16% population mortality resulting when measles first arrived on Rotuma in 1911.17 Although mass mortality on islands during measles epidemics is primarily due to the inability of people to care for the many simultaneously ill individuals, measles mortality was noted to be characteristic of rural areas likely due to social isolation. Measles mortality in the US Army correlated between the US Civil War and World War I based on geography (rurality and US state).18 The disappearance of rural isolation as part of the process of globalisation might partially explain why black measles is no longer described today.19
So, what then was black measles as seen by the US Civil War medical officers? Unless one discounts their powers of clinical observation, black measles was a form of severe measles infection that is no longer commonly seen in modern times. The most consistent explanation of the rash is that it was due to some form of cellular immune imbalance, possibly due to malnutrition in the days before anyone understood micronutrients and balanced diets. Epidemiological isolation certainly contributed to the large number of adult measles cases seen in the military until the mid-20th century. However, it seems unlikely that black measles is just a rare manifestation of adult measles. The most consistent modern clinical picture of black measles is the same viral infection in malnourished African children, often with protein-calorie malnutrition in refugee camps.13 It is, however, worth noting that such severe measles infections in refugee children during the Boer War 1899–1901 did not result in black measles but rather secondary pneumonia as the leading cause of death.20 Measles-related deaths in Rotuma in 1911 were often due to subacute ileocolitis without any particular reference to severe rashes as part of the disease.17 Systemic viral infections can result in anomalous findings in rare or abnormal hosts, likely the best explanation for black measles during the US Civil War. That one can at least partially reconstruct the history of black measles from observations that pre-dated any modern understanding of infectious diseases is a testament to the medical officers who struggled to care for their soldiers under unimaginably difficult wartime circumstances. Unusual clinical findings remain worth recording if only in the hopes that our scientific successors will better explain what we cannot currently understand.
Corresponding Author: G. Dennis Shanks, Dennis.Shanks@defence.gov.au
Authors: G D Shanks1,2
Author Affiliations:
1 ADF Malaria and Infectious Disease Institute
2 University of Queensland – School of Public Health



