
Medical corps officers were often the ‘canary in the coal mine’ for infectious disease mortality in armies during the pre-antibiotic era. This means that medical officers could be among the first indicators of a serious medical problem (See https://wordhistories.net/2018/03/31/canary-coal-mine). Deployed forces, however, could experience exotic threats, such as malaria and cholera, that could kill both soldiers and those who cared for their illnesses. Up to a third of the Ottoman Army’s medical officers died from epidemic typhus spread by lice during campaigns in Anatolia and Russia.1, 2 The Australian Army medical and nursing personnel, however, died largely of influenza and secondary bacterial pneumonia, particularly during the pandemic of 1918.3 Interestingly, although both military medical corps had very similar duties, their predominant cause of infectious disease mortality did not greatly overlap.
Australian Army data were taken from previous work to characterise the mortality during the 1918 influenza pandemic, which used detailed information on all Australians serving during World War I. These data include officers and enlisted members of the Royal Australian Army Medical and Nursing Corps throughout the entire conflict. The Turkish Army information is drawn from a published report on medical officer mortality in the Third Ottoman Army, which was largely limited to Eastern Anatolia.2 Combat-related mortality caused an estimated 70% and 10% of all-cause mortality in the Australian and Turkish Army Medical Corps during World War I. Medical understanding of specific infectious diagnoses during the early 20th century was limited, and laboratory support was often minimal. Given these caveats, a comparable number of documented medical deaths (219 vs 279) were documented and are shown in Figure 1.
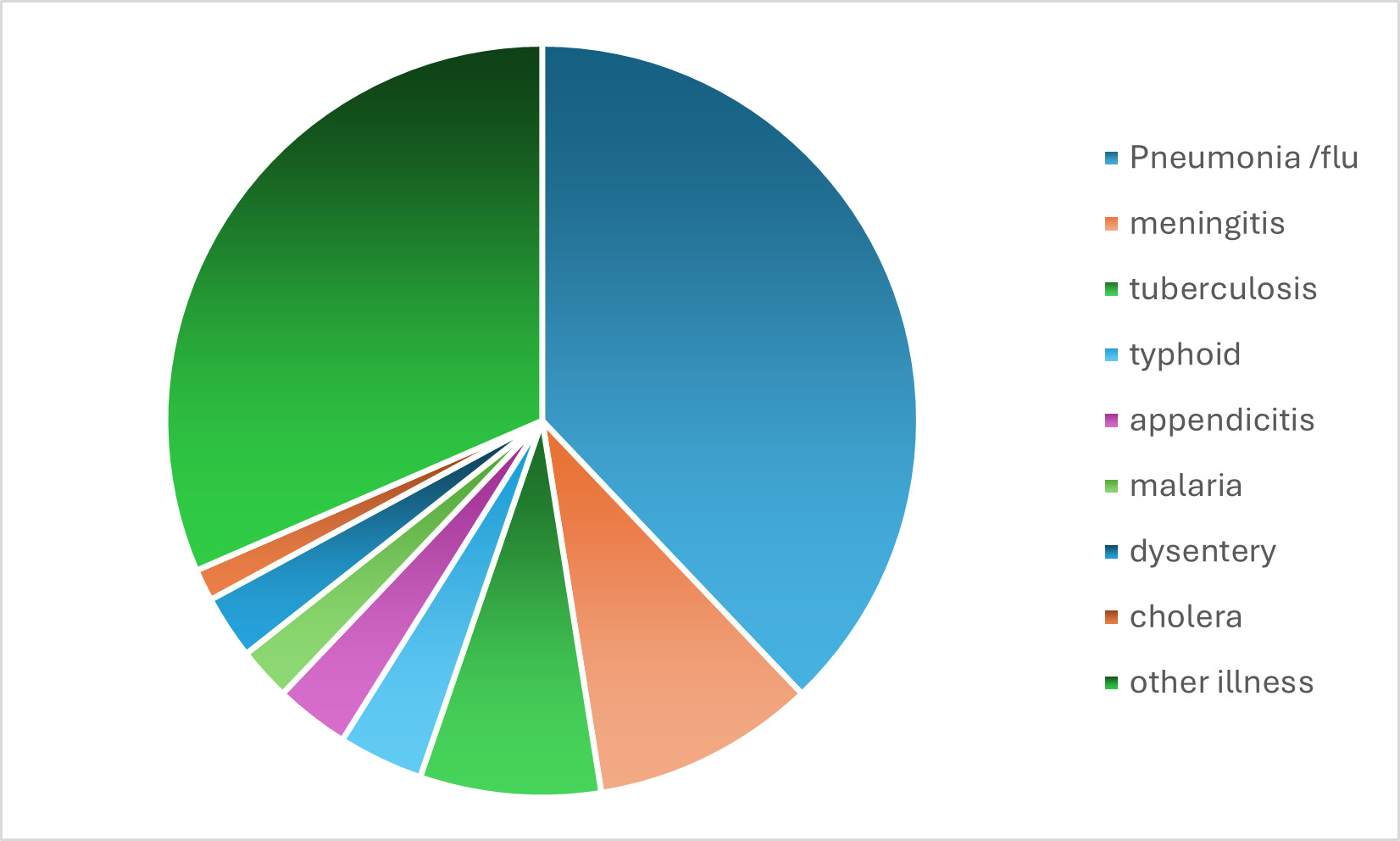
Figure 1: Medical mortality during World War I (1914–19) in the respective medical corps of (A) the Australian Imperial Force (n=219) compared to (B) the Third Army of the Ottoman Empire (Turkey) (n=279).2, 3 Note the predominance of pneumonia/influenza deaths in the Australian Army, mostly during the 1918 pandemic and the typhus deaths in the Turkish Army during campaigns in Anatolia.
Why did similar armies experience such a large difference in their predominant cause of infectious disease mortality in their medical corps? All soldiers of World War I had lice, but only some had typhus. This limitation of one of the greatest war-related epidemic diseases on the Eastern Front was likely due to the rickettsia reservoir in humans, rather than to any variability in the vector.4 Turkish soldiers were originally infected from the rodent reservoir, and then continued the cycle, while this only happened occasionally in the Australian Army.
The 1918 influenza pandemic was global in scope but highly variable in its mortality. The single greatest factor determining pandemic mortality in the Australian Army was that when a soldier enlisted as a recent recruit, they died at much higher rates than veterans.3 Turkish medical officers got influenza, but they died at very low rates, possibly because they had already developed some resistance to circulating respiratory bacteria, which were responsible for the lethal secondary pneumonias.5 Historical epidemiology of previous wars can still give useful insights into epidemic infectious diseases that are our best model for biological threats to future military operations. Hopefully, medical officers will no longer be ‘canaries in the coal mines’ of future operations.
Please specify the URL of your file


