
Abstract:
Pertussis (whooping cough) is not typically considered an infectious disease of military significance, as its most severe manifestations are primarily restricted to unimmunised children. Pertussis is increasing, particularly in Australia and the Pacific Islands, due to falling immunisation rates and the post-COVID pandemic surge in all respiratory infections. Obscure outbreaks of chronic cough in soldiers have been identified as pertussis during modern military deployments to Korea, Afghanistan and Germany, as well as during military training in the USA, France, Israel and Finland. Often, the soldiers’ illness is only discovered after a young family member is diagnosed with clinically typical pertussis, as the adult form of the disease is often noted only as a severe, chronic cough. Pertussis’ public health importance is increased by its high infectivity, spread by the respiratory route and ability to incapacitate for weeks. Increasing anti-vaccine propaganda and the vulnerability of small island nations to disease epidemics mean that the medical personnel in Australia need to be aware of the potential of pertussis to spread within military units and the need to maintain current immunisation standards.
Key words: pertussis, immunisation, military history, epidemiology
‘the hooping cough…made its appearance for the first time, causing, in conjunction with the war, … a calculated reduction of five percent of the population in a period of eighteen months.’ Erskine 1853 on Samoa as reported by McArthur.1
Pertussis, or whooping cough, caused by Bordetella pertussis, is not usually thought of as a militarily important infectious disease. Although pertussis has devastated the Pacific Islands in the past, as noted in the quote above, the introduction of immunisation from the 1930s largely confined severe forms of the disease to infants and under-immunised populations. Several factors have shifted this perception, including increased adult pertussis cases as childhood immunity wanes, anti-vaccine propaganda causing immunisation refusal/hesitancy in some populations, and multiple outbreaks during military deployments. Focal epidemics of pertussis have disrupted military operations in Afghanistan, Korea, Germany and the USA. This short review aims to highlight pertussis as a cause of chronic cough associated with military training and deployments. It seeks to sharpen diagnostic awareness and improve communication about the continued necessity of immunisation against this re-emerging respiratory pathogen.
The whole-cell pertussis vaccine (usually given in combination with diphtheria and tetanus toxoids as DTP) was immunogenic but also reactogenic, leading to its replacement in the late 20th century by an acellular pertussis vaccine based on individual protein antigens. This positive outcome had the apparent unintended consequence of producing less long-lasting immunity to pertussis in adolescents and adults. Although it is not possible to precisely estimate this decrement, an increasing number of countries have noted adult cases of pertussis in the 21st century and have responded by adding additional booster doses of diphtheria-tetanus-acellular pertussis (dTPa) to various national adolescent and adult schedules. The current Australian Technical Advisory Group on Immunisation (ATAGI) recommendations include a booster dose of pertussis-containing vaccine for all adolescents aged 11–13 years and at 50 and 65 years if no previous booster had been received in the last decade. ADF members receive dTPa boosters once a decade in addition to ATAGI recommendations to stay current with military requirements.2
In the USA, pertussis was first identified as a disease at a recruit camp in the late 1990s among US Marines in California, where there was no state requirement for an adolescent booster containing pertussis following primary immunisation.3 Pertussis is difficult to diagnose as the bacteria are often gone by the time the person presents with a chronic cough. Despite negative culture and genomic techniques, the investigators were able to implicate pertussis during an outbreak of chronic cough disease largely through serological conversions in a minority (20/120) of affected Marines.3 Often, the military context of pertussis is only appreciated when young children are diagnosed with classical pertussis symptoms (whooping) and their parents/caretakers are found to have a chronic cough. Only 10% of the pertussis cases diagnosed in the US DOD occur in active duty military members. A steady number of cases (476 confirmed) was reported from 2005 to 2012, with associated clusters in California, Texas, Florida and Okinawa.4 Pertussis during USA military deployments was considered as an explanation for the widely experienced ‘Pohang crud’ of cough illness seen commonly during military exercises in South Korea.5 Extensive diagnostic work on 54 symptomatic volunteers with more than two weeks of cough in South Korea showed a combination of infections due to pertussis, Chlamydia and Mycoplasma that were different from matched controls. Serological diagnosis was possible in many cases, again in the absence of isolated organisms; most volunteers had symptoms that limited their ability to perform their military duties.5
The French Army also experienced pertussis epidemics in the early 21st century. A military school outbreak in adolescents in 2006 was one of the first warnings that pertussis was a re-emerging infectious disease problem.6 Over 200 suspected cases (estimated attack rate 18/100) were seen in this adolescent population. Vaccine protection during the outbreak was estimated at 80% for those having had pertussis-containing immunisations within the last six years. This emphasised the importance of catch-up immunisation for those who had missed a dose at 11–13 years.6 A parallel and possibly related event in the International Security Assistance Force (ISAF) in Afghanistan also observed 200 cases of chronic cough, which included French, Greek, German, UK and other allied soldiers in Kabul.7 This also approached a 20% attack rate and 14/49 patients with chronic cough were ill enough to require hospitalisation. Given the low rates of immunisation in the Afghan population, it seems likely that the ISAF outbreak was overflow from civilians into a suboptimally immunised deployed military population. Further evidence that the ‘Kabul cough’ was not limited to Afghanistan came from the British Army’s experience in Germany, showing that cases in soldiers and their families were likely from military members returning from Afghanistan.8 Increased medical surveillance for pertussis in the French Army yielded an estimate of 35 cases/100 000 in 2007, primarily in adult men.9 A policy change was introduced in 2008 to immunise recruits with dTPa, with about 30 000 doses/year given and the subsequent reduction in cases to 14/100 000 by 2011.10 Surveillance for vaccine adverse events within the French military estimated 100/100 000 for pertussis-containing vaccine, of which only 1/100 000 were serious ones such as Guillain-Barré syndrome.11 Immunisation, especially of young men on military entry, appeared to directly address the problem of adult pertussis in the French military.
The Finnish Army also made a major change in pertussis immunisation policy within its large male conscript population.12 Acellular pertussis vaccine was introduced in 2005 in Finland and pertussis peaked at 49/100 000 in the 19–21 year old population in 2011. Subsequently, booster doses were offered to all military recruits from 2012, and pertussis rates dropped to <1/100 000 by 2015.12 The fall in pertussis rates across the entire population, including females, was felt to be indicative of herd immunity by immunising a large number of male adults. This was further evidence that the re-emergence of adult pertussis infections was due to inadequate immunisation.
In the Israeli Army, pertussis was largely seen as a disease of recruits, with 110 cases studied in 2001–03, each having a median two-week duration of cough.13 It was estimated that 23% had serological evidence of pertussis infection with an estimated attack rate of 2132 cases per 100 000 person-years. Since Israeli children were not then being immunised as adolescents against pertussis, it was likely that the recruits were insufficiently immunised. In 2015, another pertussis outbreak occurred in the Israeli military despite the introduction of booster doses containing pertussis to the general population at age 14 from 2008.14 Approximately 10% of 1500 soldiers were symptomatic, and 39% of these were shown to have evidence of pertussis infection. Post-exposure antibiotic prophylaxis was given to terminate the outbreak, but it was unclear if additional pertussis immunisation was added to the Israeli Army policy, given the objections of some Orthodox Jewish groups in the conscript military force.14 Conscript forces such as Israel and Finland, differ from all volunteer forces (UK, Australia) in that they cover a broader population whose immunisation status is heavily dependent on the public health system from which the citizen soldiers are drawn.
The current situation in the ADF is that occasional cases of pertussis are diagnosed within the military population, but there have been no recent epidemics. Pertussis is clearly resurging in Australia after the pandemic-induced lockdown pause in many respiratory diseases. See Figure 1, which shows record numbers of pertussis cases (>50 000) in Australia in 2024. Although upper respiratory infections are always a major chief complaint of deployed soldiers, medical officers need to be aware of the epidemiological situation and ready to bring in more advanced genomic diagnostics when indicated by unusual patterns of disease. The regional situation is similar in that pertussis is increasing in New Zealand, Hawaii and French Polynesia with reports of transmission in New Caledonia.15 Given the fragile state of many small Pacific Island health services and the ease of travel from known areas of infection, such as Australia, pertussis outbreaks would seem to be highly likely on Pacific Islands in the near future. Whether this would produce a crisis similar to the Samoan measles epidemic of 2019 is unknown. However, the ADF might be called to respond along with other international organisations to such a humanitarian assistance disaster recovery mission.16
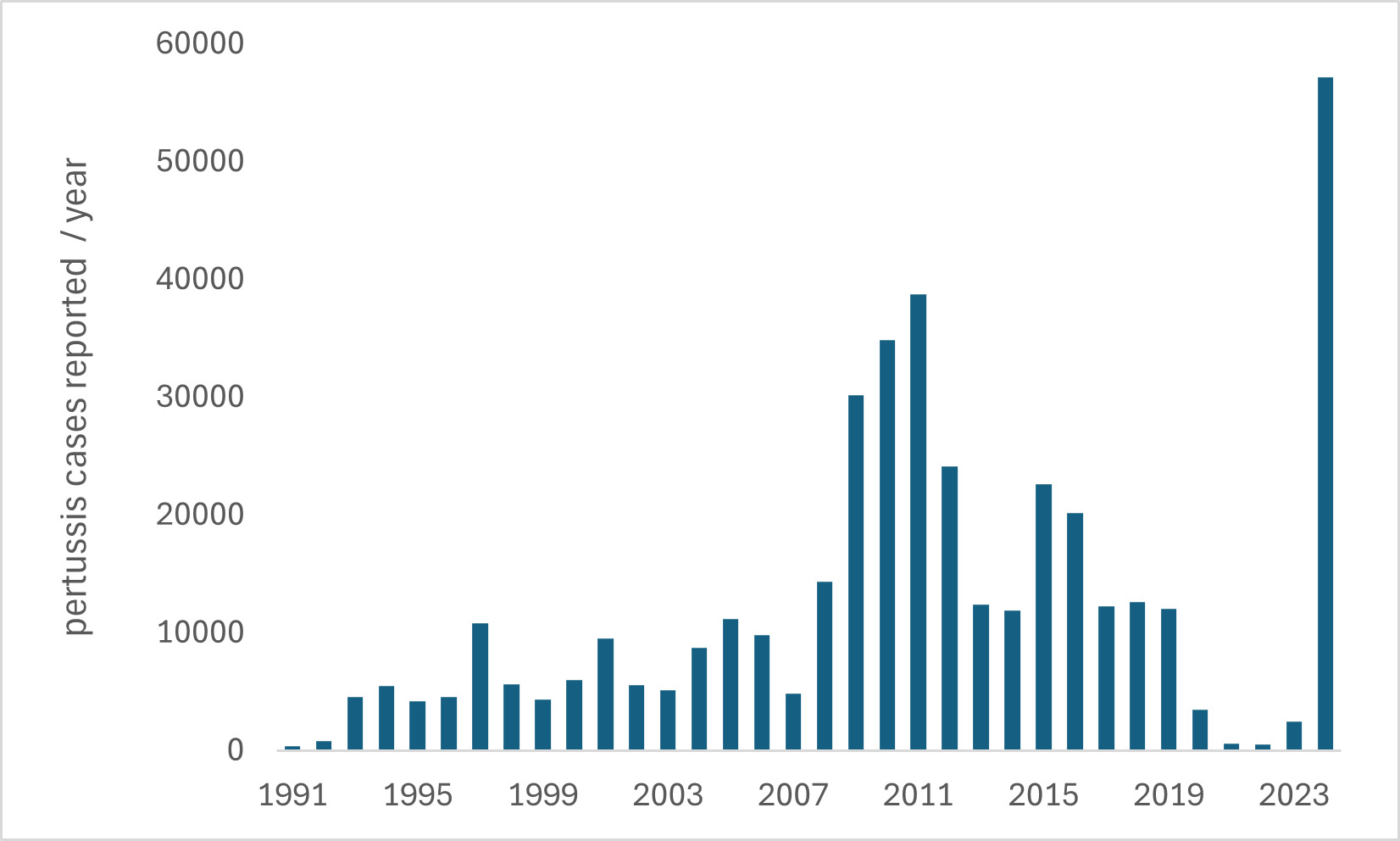
Figure 1: Pertussis cases reported in Australia by year based on data from the National Notifiable Disease Surveillance System https://nindss.health.gov.au/pbi-dashboard, noting the relative gap during the COVID pandemic 2020–2022 when all respiratory infections decreased due to restrictions in population movement.
Pertussis is a highly infectious respiratory infection that has shown its ability to cause epidemics in military populations, which are difficult to recognise and treat. The operational consequences of undocumented pertussis are primarily observed in extended illness and the inability of deployed soldiers to fully function. However, naturally occurring infectious diseases can sometimes become the source of rumours and disinformation, which can synergistically harm unit effectiveness and cohesion. The rise in anti-vaccine propaganda and resulting vaccine hesitancy is likely to increase, given the recent high-profile removal of mandatory COVID vaccines in the US military.17 There is sufficient experience from the French, Finnish and Israeli Armies to indicate that pertussis prevention is a matter of maintaining sufficient adult immunity with pertussis-containing booster injections. The current policy of administering such immunisations each decade needs to be defended. The ADF should not be forced to demonstrate that it is no different from other larger military organisations that learned about pertussis through epidemics when immunisations failed to maintain soldiers’ immune status.
Author affiliations: Australian Defence Force Infectious Disease and Malaria Institute, Gallipoli Barracks, Enoggera, Queensland, Australia
University of Queensland, School of Public Health, Brisbane, Herston, Queensland, Australia
Funding: No specific funding was provided for this work. The author is an employee of the Australian Defence Force, a retired US Army officer and claims no conflicts of interest.
Disclaimer: The opinions expressed are those of the author and do not necessarily reflect those of the Australian Defence Force or the US Department of Defence.



