
Abstract:
Future armed conflict in the Indo-Pacific region may see small detachments of soldiers deployed on isolated Pacific Islands for extended periods. Historical experiences with such deployments, particularly during World War II, are reviewed to give insight into possible medical problems and their countermeasures. The 8th Division of the Second Australian Imperial Force (2 AIF) is infamous for its experiences on the Thai–Burma railway. However, it also contained three separate one-thousand-soldier detachments which Imperial Japanese Forces destroyed on New Britain, Timor and Ambon. Crisis mortality (2%/month) was associated with cholera epidemics and forced labour periods under conditions with little food and many tropical infections, such as malaria. Many POW deaths were due to ship sinkings by Allied submarines. Some isolated garrisons, such as a Japanese Naval Battalion on Nauru, survived well until post-war repatriation exposed them to epidemic malaria. Medical preparations for isolated island garrisons need to focus on supplies of fresh water and rations, pre-deployment immunisation and chemoprophylaxis against scrub typhus and malaria. Lack of medical evacuation may present significant practical and psychological challenges for isolated island deployments in a future conflict.
Keywords: military, mortality, Pacific Islands, historical epidemiology
I find it difficult to overcome a feeling of disgust, and more than a little concern at the way in which we have seemingly been ‘dumped’ at this outpost position. LTCOL Roach, Ambon 19421
Geography often determines what is possible during armed conflicts. If war occurs in the South China Sea, a range of Pacific Islands will be involved, some of which may be held by small detachments of soldiers who will purposefully be isolated from direct support due to the extreme risk to any resupply or evacuation missions. This tenuous logistical chain is very different from most recent conflicts. One needs a historical perspective back to World War II to anticipate what might occur during future Pacific Island deployments. Detachments of the 8th Division of the 2 Australian Imperial Force (2 AIF) containing individual infantry battalions were posted to New Britain, Timor and Ambon in 1942. All were quickly overwhelmed and destroyed by the Imperial Japanese offensive.1,2,3 It seems very likely that any future regional deployments will be small and inconspicuous to avoid such a fate. So, the question becomes, how does one medically prepare a company-sized unit for an extended and possibly indefinite stay on small Pacific Islands? Although infectious diseases such as malaria and scrub typhus have been critically important in the past, other types of casualties, particularly psychological, will likely be important in determining mission success in the future. We can try to anticipate the future, but this analysis is based on the past, as this brief historical review is taken from casualty figures primarily from the Official Histories and the Commonwealth War Graves Commission.
New Britain, Papua New Guinea:
The 2/22nd BN formed most of the fighting strength of Lark Force on Rabaul in New Britain.3 Most of the force were captured around Rabaul after the Japanese amphibious invasion of 23 January 1942, but about 400 soldiers escaped capture, evading along the coast of New Britain.4 About 160 Australian soldiers who could no longer flee were massacred by Japanese soldiers of the 1 / 144th Infantry Regiment at the Tol Plantation. Nearly all the survivors developed malaria during their trek in the jungle, and it is estimated that 20% of them died of malaria when the medical officer ran out of quinine.5 Eventually, 156 survivors were evacuated by the HMAS Laurabada to Finschhafen. It is estimated that only four hundred escaped out of a mixed military force of 1396 in Rabaul; barely a quarter of the 22nd Battalion survived the war. Most (849) of the remaining Prisoners of War (POWs) from Rabaul died when a US Navy submarine sank the Montevideo Maru off Luzon in Philippines on 1 July 1942.4 Even the pursuing Japanese soldiers did poorly with at least 5% of the 1/144th Regiment dying of malaria on New Britain prior to their transfer to Kokoda Campaign where the unit was destroyed.6,7
Timor and Ambon, Indonesia:
The 2/40th BN was the core of Sparrow Force in Kupang, Timor and Dili in Portuguese East Timor.2 A Japanese amphibious and airborne assault cut off the Australian and Dutch Forces on Timor, leading to most becoming POWs in February 1942, many being transported to Thailand or China. Eighty per cent of those remaining in the field were estimated to have malaria within a month. The 2/2 Independent Company AIF was able to conduct guerrilla operations until the end of the year, when it was withdrawn exhausted as it could no longer be supplied without unacceptable shipping losses from Darwin.8
The 2/21st BN was the infantry component of Gull Force on Ambon in the Netherlands East Indies (now Indonesia), originally commanded by LTCOL Roach, whose quote is shown at the beginning of this article.1 Gull Force and Allied Dutch soldiers were overwhelmed by a Japanese amphibious assault backed by aircraft carriers on 24 February 1942. It is estimated that 800 Australian soldiers surrendered and that the Japanese massacred 300 around Laha airfield. Of the 532 survivors, 405 died in captivity of starvation and disease. Only about 300 members of Gull Force survived the war.9
Prisoners of War:
Due to the circumstances of the comprehensive Allied defeat in 1942, with few surviving records, it is difficult to make detailed observations on POW mortality. Post-war information reconstructed by the Commonwealth War Graves Commission from Allied medical officers serving on the Thai–Burma railway provides sufficient data for the illustrative graphs.10 Figure 1 shows that Allied mortality in Singapore was limited mainly to the combat phase prior to capture. Those soldiers staying in Singapore had relatively low mortality, consistent with other prison situations. In contrast, those POWs sent to the infamous Thai–Burma railway died in large numbers from malnutrition, mistreatment and tropical infections. Crisis mortality rates peaked at 2% per month in mid-1943 during cholera epidemics, repeated malaria episodes and overwork forced by the Japanese to complete the railway construction in October 1943.11,12 Figure 2 shows that mortality on the Thai–Burma railroad in 1944–45 was relatively low, many of the weaker soldiers having already died during the railroad construction. Soldiers over 35 years died at a rate consistent with their proportion of the force. Officers and medical personnel were relatively spared, mainly because most were exempted from construction labour. Most sick POWs survived the war period if they remained in Thailand due to hospital camps offering surgical care, including life-saving blood transfusions from fellow POWs for chronic relapsing malaria.13 Malaria was thought to be the direct cause of 4% of POW deaths and indirectly killed another 7%.11 Scrub typhus was described as jungle fever and likely killed some POWs due to the absence of antibiotics. However, the leading causes of mortality were gastrointestinal infections, malnutrition, especially beriberi and chronic skin ulcers.14 Mass mortality events accelerated overall mortality during submarine sinkings of ‘fit’ men shipped to Japan. It is estimated that 10 000 Australian soldiers of the 8th Division died during World War II, or two-thirds of all Australian war dead in the Pacific theatre.10
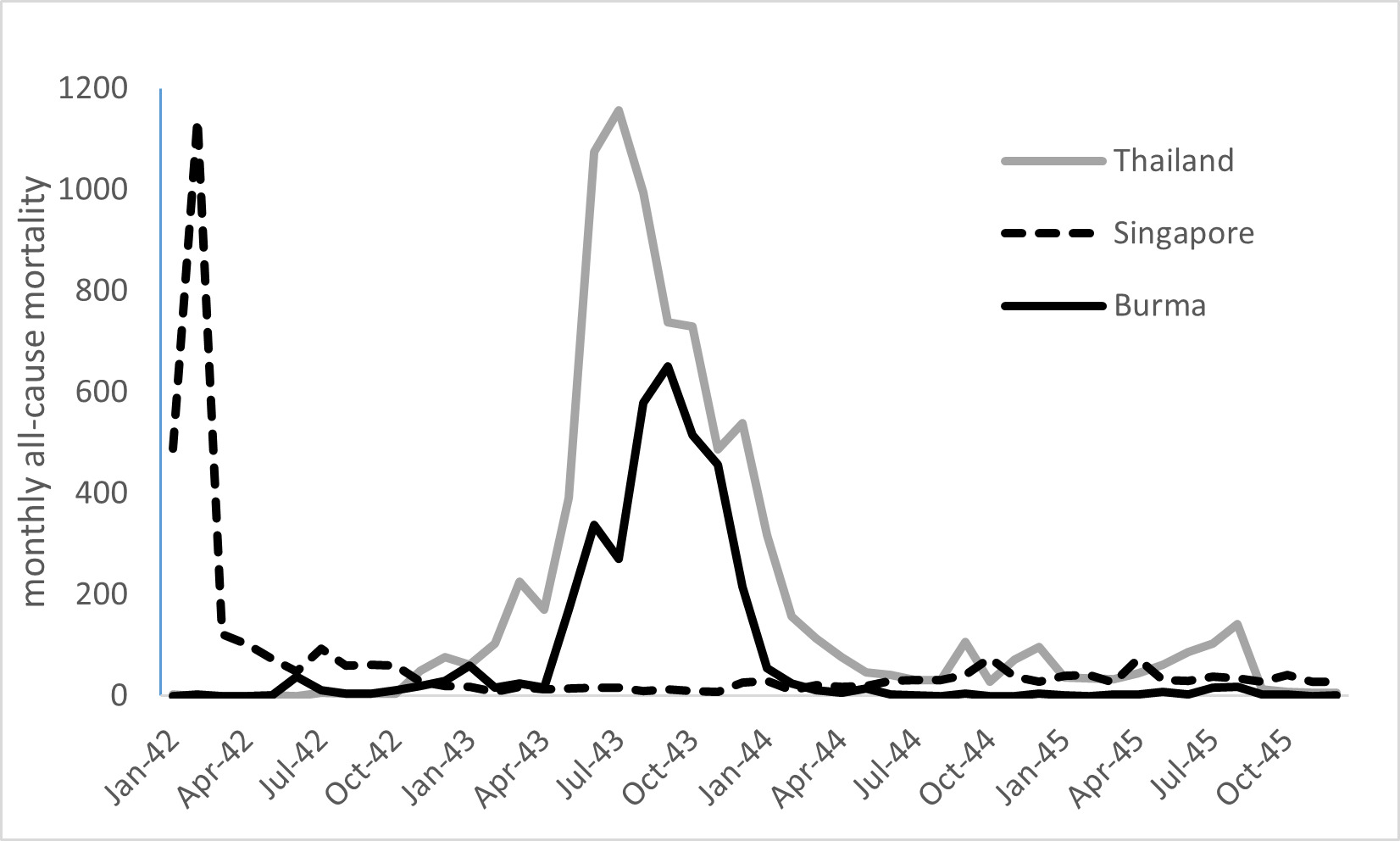
Figure 1: Statistics compiled from the Commonwealth War Graves Commission (https://www.cwgc.org/) for the Thai–Burma railway and Singapore cemeteries. All-cause mortality is shown, with the vast majority of combat deaths seen in Singapore prior to March 1942.
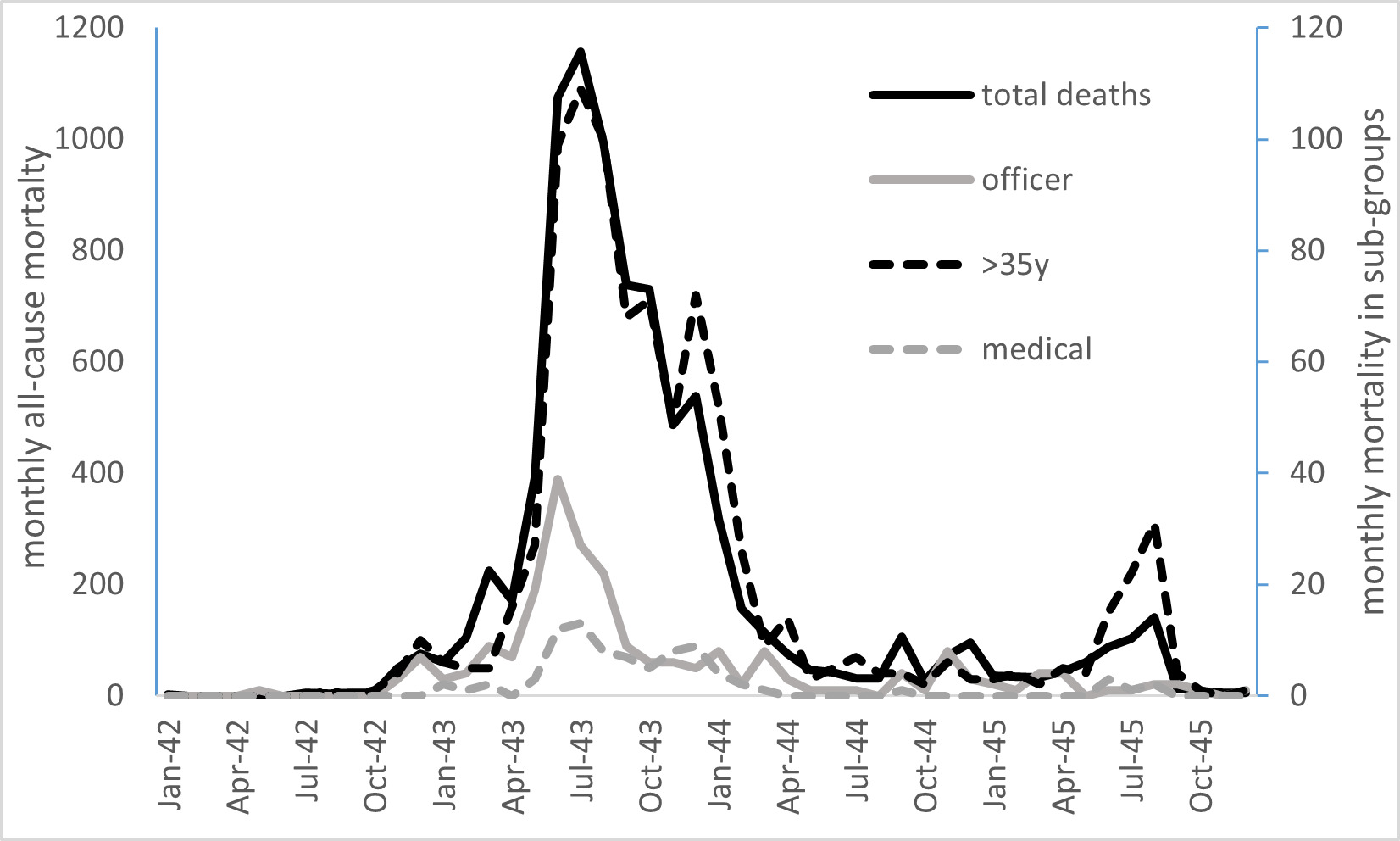
Figure 2: Statistics compiled from the Commonwealth War Graves Commission (https://www.cwgc.org) for the Thai–Burma railway and Singapore cemeteries. Total deaths shown with peak mortality of approximately 2%/month in mid-1943. Note that officer, medical personnel and soldiers >35 years mortality is shown on the right axis at one-tenth the scale of the left axis.
Other Pacific Islands:
Other isolated garrisons in the Pacific were illustrative of specific infectious diseases. Bat Island, south of Manus, Papua New Guinea, was occupied by a joint Australian/USA observation unit of 41 men in 1944.15 Within six weeks, scrub typhus had killed two and 26 others were sick (68%). The island, meant as a strategic weather/surveillance site, was abandoned as uninhabitable due to the large rodent reservoir of scrub typhus, a disease which was untreatable at the time. The Japanese Naval Battalion on Nauru Island was bypassed by the war, except for long-distance bombing raids.6 Eight hundred men were transshipped to the Solomon Islands post-war camps in preparation for repatriation to Japan. Within two months of their October 1945 arrival, two-thirds of the Japanese had been hospitalised and 27% had died of epidemic falciparum malaria despite treatment in Australian-supplied, Japanese-run hospitals in the Shortland Islands. Malaria does not occur in Nauru due to the lack of an Anopheles vector, and the fact that these otherwise well Japanese prisoners were at severe risk of malaria was overlooked in the process of repatriating many thousands from New Guinea/Solomon Islands.5
Another major Australian military repatriation mission on Muschu Island collected the remnants of the Japanese 18th Army. It is estimated that 79% of the 18th Army did not survive the war, the vast majority due to starvation and infection, not combat losses.16 Even after surrender to Australian forces in Sept 1945, 1008 of 13 000 Japanese survivors succumbed to illness despite Allied logistical efforts to provide food and medicines.17 Figure 3. Like those on the Thai–Burma railway, their deaths were due to a composite of starvation, malnutrition (beriberi) and chronic infections with a variety of tropical diseases. Garrisons cut off from logistical supplies with minimal medical support did very poorly, whether Allied or Japanese.16

Figure 3: Captain L. Keeley RAAMC examines a sick Japanese soldier surrendered on Muschu Island, New Guinea, in late 1945. Many sick soldiers died after the surrender due to the combined effect of starvation and infection over many months in the New Guinea jungle. Photo 019273 Australian War Memorial now in the public domain.
Conclusions:
If future conflicts necessitate the deployment of detachments of soldiers on isolated Pacific Islands, some general statements and warnings can be made, assuming one is dealing with small units that are trying to remain hidden from the enemy. Uninhabited islands have no population for a reason, usually a lack of fresh water supplies. Careful thought needs to be given to drinking water supplies (desalination, coconuts), as it will be impossible to stockpile large amounts of water in a concealed manner. Drinking water is truly a non-negotiable logistics item, and history is replete with units made ineffective by using non-potable water sources. Soldiers can exist on minimal rations for several weeks, if necessary, but several World War II garrisons truly starved. POWs were very inventive in finding nutritional sources in tropical Asia, but that may not be possible on small coral islands. Fishing gear and supplemental vitamins to prevent deficiencies, such as beriberi, may be able to address the lack of other food supplies. Medical personnel will be limited to the unit medic, who will need to be very confident about independent medical decision-making, as it will not be possible to use telemedicine due to the need to suppress all electronic signatures. Medical evacuation will only be possible when missiles cease at the end of the conflict, necessitating consideration of methods to mark, record and respectful inter soldiers who die until their remains can be recovered later. Scrub typhus is likely to be a problem on small islands in the South China Sea.18 The main regional malaria risk involves any of the major islands around New Guinea.19 Doxycycline is a good preventive measure for both. However, weekly tafenoquine should be considered for highly malarious areas when soldiers are expecting weeks and not just days of night-time exposure. Lack of a cold chain will limit immunisations to pre-exposure use; therefore, planning similar to that used today for Special Forces on remote duty, with special consideration for Japanese encephalitis and rabies vaccines, should be employed. Psychological casualties are common in any war, but are likely to increase when soldiers who grew up with a mobile phone are suddenly disconnected from electronic media for months.20 Based on this historical data from New Britain, Timor and Ambor in 1942, the ADF must be better prepared for the next Indo-Pacific conflict, and its medical officers should soberly consider what a high-casualty conflict would necessitate.
Author affiliations: Australian Defence Force Infectious Disease and Malaria Institute, Gallipoli Barracks, Enoggera, Queensland, Australia
University of Queensland, School of Public Health, Brisbane, Herston, Queensland, Australia
Funding: No specific funding was given for this work.
Disclaimer: The opinions expressed are those of the author and do not necessarily reflect those of the Australian Defence Force or the US Department of Defence.
Conflicts of interest: The author does not claim any conflicts of interest.
Corresponding Author: G. Dennis Shanks, Dennis.Shanks@defence.gov.au
Authors: G D Shanks1,2
Author Affiliations:
1 ADF Malaria and Infectious Disease Institute
2 University of Queensland – School of Public Health



