
Abstract
Introduction: Military service members encounter numerous stressors post-deployment. Unit cohesion, community, social connections and leadership can serve as resilience support systems and may help improve service members’ wellbeing. This research examines the perceived value of these support systems for service members post-deployment. Methods: A cross-sectional convenience sample of 78 United States military officers (n=54) and enlisted personnel (n=24) who had deployed to Iraq and/or Afghanistan completed post-deployment assessments. They were administered the Deployment Risk Resiliency Index, the Social Support Questionnaire and the Work-Life Well-Being Inventory. Results: Unit support at post-deployment predicted positive wellbeing. The nuclear family was the primary support system for service members, with extended family providing additional support post-deployment. Spouses were the most preferred support person, followed by parents, friends, siblings and children. Service members reported that effective leaders supported their individual wellbeing through communication, while ineffective leaders overworked personnel, thereby negatively affecting their personal wellbeing. Family wellbeing was supported by leaders who granted time off, whereas ineffective leaders were described as demanding, negatively affecting family wellbeing. Conclusions: The unit and leaders can contribute to these service members’ wellbeing. The nuclear family, extended family and friends are support systems identified by this sample, which largely consist of senior officers.
Key words: family, post-deployment, service member, social support, wellbeing
Key messages
- What is already known on this topic: Service members face significant stressors post-deployment, and social support plays a crucial role in their wellbeing.
- What this study adds: This study identifies unit support and leader behaviour as important sources of post-deployment emotional wellbeing in a sample that largely consists of senior officers. The nuclear family (e.g., spouse and children) was identified as the most significant source of support in this preliminary research. Others recognised as important in the service member’s support system were parents, friends and siblings in this predominantly senior officer population.
- How this study might affect research, practice or policy: Findings emphasise the need for further research on support systems, leadership training, structured family support programs and policies that strengthen unit cohesion to enhance service members’ post-deployment adjustment. Future research should develop and/or refine the measures for the Military Family Fitness Model’s demands, resources and outcomes for service members’ wellbeing. Specific to this paper, the external resources are unit support, community and social support and leadership influences.
Resilience is described as positive adaptation to adversity and is a psychological phenomenon, along with wellbeing, that consists of hedonic and/or eudemonic components and is used to train military personnel.1 The United States (US) military has invested in resilience and wellbeing resources for service members prior to and post-deployment.1 Extensive combat exposure may result in the need for service members to seek supports to address negative health impacts, specifically clinical treatment for conditions that may affect deployability (e.g., posttraumatic stress symptoms, depression and suicidal ideation).2,3 However, external support resources that are easily accessible to the individual service member—such as the nuclear (e.g., spouse, children) and extended family (e.g., parents, siblings)—may serve as an early non-clinical intervention to mitigate the possible stress related to military deployments.4 Conceptual frameworks, such as the Military Family Fitness Model, can be used to understand how service member resilience is developed, which external resources influence service member wellbeing, and what outcomes are associated with resilience and wellbeing after successful military deployments.
The Military Family Fitness Model
The Military Family Fitness Model (MFFM) is a conceptual framework that captures the complex processes involved with service member resilience. Based on the theoretical underpinnings of demands and resources, individual, family and external resources mitigate demands and influence outcomes. Specifically, the MFFM posits that external resources (i.e., unit support, community resources, social support, and leadership influences) foster resilience in service members and their families. This demand resource model provides a comprehensive theoretical basis for identifying external resources that may mitigate deployment stressors for service members and their families.4,5 The MFFM captures mechanisms at work that contribute to service member resilience and readiness, fostering adaptive outcomes (e.g., holistic health, positive relationships) and preventing or mitigating maladaptive outcomes (e.g., dissatisfaction, conflict, abuse). Adaptive outcomes, such as wellbeing and functioning, demonstrate service members’ resilience and readiness for deployment. In contrast, family fitness maladaptive outcomes (e.g., conflict, increased use of health care) are considered vulnerabilities during and post-deployment. Figure 1 provides an overview of the integrated relationship between demand, resources and outcomes.
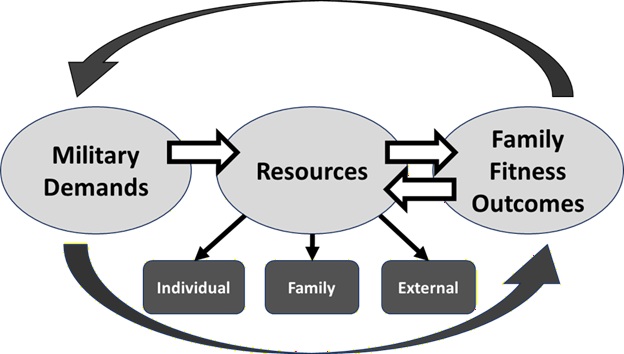
Figure 1. Military Family Fitness Diagram
MFFM external resources
The MFFM was developed as an integrated model of resilience building for both service members and military families. Based on a US military program, Total Force Fitness,4 the processes in the MFFM function on the key assumption that resilience can be learned, specifically in response to adverse or traumatic situations. Although the MFFM recognises the daily struggles unique to service members and their families, the MFFM can be particularly useful throughout the deployment cycle. Specifically, demands during and post-deployment on service members and their families require access to any and all sources of resilience. In contrast, opportunities to proactively strengthen resilience and fitness prior to deployment are greatest during and after deployment since service members are at their most vulnerable to psychological and physical threats that may result in deployment-related trauma. As conceptualised in the MFFM, external resources may mitigate and alleviate these adverse experiences. These external resources that may support service members’ resilience include unit support, community resources, social supports (e.g., family members) and leadership influences.
Unit support
Unit support and cohesion during deployment and post-deployment can protect against negative psychological impacts such as depression or suicidal ideation.3 Cohesive units exhibit more self-reported resilience and reduced mental health stigma, resulting in service members who identify and seek help for their needs more effectively.6,7 However, the protective effects of unit cohesion against negative psychological impacts can vary in efficacy depending on the unit cohesion dynamic. High levels of horizontal (peer-to-peer) cohesion significantly protect against post-traumatic stress symptoms (PTSS), depressive symptoms, and suicidal ideation and these effects are strongest for post-deployment depression.8 Unit-level vertical cohesion (i.e., leader to subordinate) is not as effective in mitigating the psychological effects of combat exposure, suggesting that buffering effects involving vertical cohesion may depend on the type of unit or leader.8 Past research found that greater levels of perceived unit cohesion were related to a decrease in behavioural health symptoms, therefore serving as a buffer to stress in the military environment.9,10
Community resources
Military OneSource can offer service members community resources to help mitigate challenges associated with returning home.11 For example, community programs, such as peer support groups,12 offer important non-clinical services that service members might find more accessible, as they may avoid traditional mental health resources due to stigma.7 These groups can offer purpose development, meaning making and normalisation of struggles.13 Nature-based recreation therapy is effective in strengthening interpersonal skills.14 Additionally, membership and engagement with a Veterans Service Organization (VSO) is linked to reduced social isolation and greater perceptions of benefits by veterans post-deployment, both of which are associated with lower levels of post-traumatic stress symptomatology and improved health.15
Social support network
Social connections improve service members’ ability to cope with military demands, enhance overall wellbeing and build an identity outside the military, thereby increasing their satisfaction with life.16 Support originating from the family and non-military friends improves dyadic functioning, and this improvement in the relationship is associated with decreased psychiatric symptoms (e.g., PTSS, depressive symptoms, and anxiety) and has a significant effect on PTSS even after accounting for prior stressors.2,5 The presence of social support from family, peers and the community is also associated with increased global psychosocial functioning and resilience.6 Moreover, service members’ perception of social support has been found to influence the effects of post-deployment PTSD symptoms.17
Leaders influences
Service members’ ability to garner support from their families can be impacted by their leaders and work circumstances, which can impact overall wellbeing.18 Supportive leadership may enhance service members’ wellbeing; for instance, sharing the training calendar to provide for planning ahead for family events months in advance.19 Leaders who engage in family-supportive supervisor behaviours such as providing emotional support, role-modelling and creating work–family management support, help subordinates balance stressors and reduce work-to-family spillover.20 These types of supervisors also have a positive impact on emotional wellbeing and stress reactivity.21 Support from work supervisors is negatively associated with psychological distress.22
Current study aims
This research examines external resources that support service members’ resilience during and post-deployment. The current study extends the conceptual framework of the MFFM. The study’s research aims to measure RQ1 unit support, RQ2 community resources and RQ3 social support for service members who have deployed. An additional aim for the research team was to qualitatively describe the effectiveness of RQ4 leadership influences perceived as an additional external resource for post-deployment wellbeing. Specifically, this research sought to address the following research questions (RQ):
RQ1: How does unit support function as a source of resilience for service members during and post deployment?
RQ2: How does community support function as a source of resilience for service members returning from deployment?
RQ3: How do service members rank nuclear and extended family members as social support resources associated with resilience?
RQ4: How do service members describe the influences of their leaders on their wellbeing and the wellbeing of their family?
The current study focused on a small population that overrepresented—but was not exclusive to—highly educated, male, white senior officers. While this is a limitation, it also provides a unique insight into the demands of the deployment cycle on those service members and their families, the resources required to meet these demands and the outcomes that may be expected due to the challenges and adversities experienced during and post-deployment.
Method
Participants
After obtaining institutional review board approval, recruitment for this study occurred at two installations in the eastern US. To be eligible for the study, service members had to be married and have been deployed within the last five years to combat zones (Operation Iraqi Freedom [OIF] conflict in Afghanistan from 2001–2013 and/or Operation Enduring Freedom [OEF] conflict in Iraq from 2003–2011). Seventy-eight service members from the US Army (n =34), Air Force (n =14), Navy (n =11) and Marine Corps (n =16) participated in this cross-sectional study from 2011-2013. Surveys were completed in person at the aforementioned installations in east-coast regions of the US. The majority of the sample identified as Caucasian (82.1%), with 27.9% selecting a minority race/ethnicity (from options including Black, Indian, Caucasian, Alaskan, African immigrant, Asian, West Indian, Pacific Islander, Don’t know and Other). Of the participants, 87.2% identified as male (n =68) and 69.2% of those were officers (n =54). Over half of the sample (62.8%, n =49) had completed college. The average age of the sample was 39.75 years (SD =7.83), reflecting a predominantly senior officer demographic (O5-O6) with greater educational attainment.
Compared to participants in the current study, 30.4% of the US military comprises service members who have identified with a minority race/ethnicity (including Black or African American, Asian, American Indian or Alaska Native, Native Hawaiian or other Pacific Islander, Multiracial or Unknown). The slight underrepresentation of racial and ethnic minorities in this sample is also reflected in a slight underrepresentation of female service members, who make up 19.3% of the US military. The underrepresentation of enlisted personnel is more significant, reported at 81.8% as of 2023.23
Although these differences in participant composition and sample representation may limit the generalisability of the results to service members from minority groups or to younger, predominantly enlisted populations, they contextualise the findings within a more experienced segment of service members. However, this oversampling of military officership and experience provides a novel perspective on external resources for resilience building during and post-deployment.
Measures
Currently, no single instrument is available to measure the MFFM. The research team selected the following measures, which have demonstrated construct and measurement validity to investigate each research question.
Deployment Risk and Resilience Inventory
The Deployment Risk and Resilience Inventory (DRRI; α =0.94) is a broad measure of risk and resilience factors related to military deployment.24 Several subscales were adapted to include post-deployment measurement.
Unit support during deployment
Section F of the DRRI consists of 12 items (α =0.88) that measure unit camaraderie, leadership and a sense of belonging within the military community to assess perceived support during deployment. Participants selected their level of agreement with statements such as, ‘While deployed, I felt a sense of camaraderie between myself and other soldiers in my unit’.
Unit support post deployment
This 12-item measure is a modified version of the DRRI Section F, modified to assess unit support post-deployment. Items (α =0.92) mirror the DRRI Section F for the post-deployment time frame, that is, ‘After deployment, I felt a sense of camaraderie between myself and other soldiers in my unit’.
Post deployment social support
Section L of the DRRI consists of 15 items (α =0.83) that assess the social support service members receive from friends, family, work associates (i.e., supervisors, peers) and the general public post-deployment. Section L also includes items that reference community support. Participants select their level to which they agree with statements such as, ‘The American people made me feel at home when I returned’.
Social Support Questionnaire
The Social Support Questionnaire (SSQ) examines six dimensions of social support.25 Participants selected responses that capture their perceived support in these areas (e.g., when tense, when feeling down, etc.). Respondents were asked to rank (1–9) who they received the most support from, with 1 being the person who provided the most support. The scoring procedure averaged frequency across the six domains of social support. Since the SSQ ranking is ordinal, calculating Cronbach’s alpha to establish reliability was not necessary.
Work-Life Well-Being Inventory
The Emotional Well-Being (EWB) subscale of the Work-Life Well-Being Inventory (WLWBI) comprises five items (α =0.71) that assess emotional wellbeing (e.g., optimism, a good sense of humour).26 Leadership influence was examined through four open-ended questions (Appendix A) that asked participants to share three effective and three ineffective actions of their leaders to support individual and family wellbeing and to rank their responses by order of importance.
Data analysis
This exploratory measurement of the MFFM required both parametric and nonparametric analyses due to the small sample size and the combination of quantitative and qualitative responses.
Unit support and community resources
Regression models were fit to answer the first two research questions, with emotional wellbeing configured as the dependent variable, measured by responses to the EWB-WLWBI. For research question one, responses to DRRI Section F regarding unit support during and post-deployment were analysed to compare means. To answer research question two, responses to the DRRI Section L regarding community resources were configured as the predictor variable for service member wellbeing, again measured by the EWB-WLWBI.
Social support
To answer research question three, quantitative and qualitative data from each of the six SSQ subscales were collected to identify sources of social support associated with service member resilience. To examine support person categories across the subscales, the counts and ranking positions of the endorsed support categories were totalled, regardless of ranking position. The total for each subscale was then added together to create a total frequency and score. Qualitatively, the responses were condensed into similar categories. Responses were nuclear family, extended family or non-family members to identify the highest-ranked support person for each subscale. ‘Nuclear family’ included spouses, children and pets, while ‘extended family’ included siblings, grandparents, aunts and uncles and stepfamily members. The highest-ranked self-reported support persons were extracted to complete this analysis. Additionally, the frequency of each individual within each family and non-family category was analysed using Wilcoxon Signed-Rank tests (Tables 2 and 3). The percentages of endorsements and ranks were produced to examine distributional differences. Since the data is ordinal, they do not satisfy the assumptions of ordinary least squares regression. Instead, nonparametric tests were used. Specifically, the frequency of each individual within each family and non-family support category was analysed using the Wilcoxon Signed-Rank tests. All reported statistical significance was set at α =.05. Recommended thresholds were followed for small (R2 =.01), medium (R2 =0.09), and large (R2 =0.25) effect sizes.27
Leadership influence
Data on external support from leaders were collected to answer research question four by identifying leadership influences on service members’ individual wellbeing, as well as their families’ wellbeing. The responses were ranked by their effectiveness or ineffectiveness in influencing wellbeing. Responses on leadership influences on individual and family wellbeing were thematically analysed by two independent raters, who separately agreed on the final categorisation. Ranking was used to generate numerical scores in accordance with established survey research practices.28
To analyse participant ranking data, a linear weighting approach was implemented, similar to rank-sum approaches and Borda Counts used to represent relative importance, as established in decision-making research. The percentage weighting procedure used in this study emphasised the proportional importance of each major ranking category.29 Responses were weighted according to rank position (1st =3 points, 2nd =2 points, 3rd =1 point). Weights were not changed if a participant only gave one or two responses instead of all three.
Multiple participants frequently listed similar responses (e.g., ‘communication’ analogous to ‘check-ins’), so the number of points assigned to a given category was totalled. The total number of points (‘Score’) for a thematic category was then divided by the total number of points across all responses to the question and multiplied by 100 to yield a weighted percentage of total points allotted to that category in response to the question (‘Score %’).
Results
RQ 1 and 2: Unit support and community resources
Unit support for the service members during deployment did not significantly predict emotional wellbeing, F(1, 71) =0.82, =0.01, p =0.367, (95% CI -0.059 to 0.158), demonstrating a small effect size (Table 1). In contrast, unit support for service members post-deployment significantly predicted emotional wellbeing, F(1, 69) =5.67, =0.08, p =0.020, (95% CI 0.015–0.167). Unit support was positively related to emotional wellbeing, such that every one-unit increase in reported unit support predicted an increase of 0.09 in the EWB-WLWBI score. Community support for service members at post-deployment did not significantly predict emotional wellbeing, F(1, 71) =1.56, =0.02, p =0.215, (95% CI -0.036 to 0.156).
Table 1Regressions predicting emotional wellbeing
| HO | Variable entered | M | SD | B | β | R2 | F | DF | Sig |
| 1 |
DRRI- During deployment unit support |
28.22 |
8.11 |
0.049 |
0.107 |
0.011 |
0.823 |
(1,71) |
0.367 |
| 2 |
DRRI- Post-deployment unit support |
44.18 |
11.79 |
0.091 |
0.276 |
0.076 |
5.667 |
(1,69) |
0.020* |
| 3 |
DRRI- Post-deployment social support |
60.29 |
10.50 |
0.060 |
0.147 |
0.022 |
1.563 |
(1,71) |
0.215 |
Notes. * p < 0.05, ** p < 0.01, *** p < 0.001.
RQ 3: Family as social support resources
Service members listed spouses, mothers, fathers, children, brothers, sisters and friends as primary sources of social support. There was a significant difference in both the ranking and the frequency of the nuclear family compared with other social support persons (p < 0.001 for all SSQ subscales; Tables 2 and 3). There was also a significant difference in both frequency and ranking when comparing the nuclear and extended family against non-family members (p < 0.001 for all SSQ subscales; Tables 2 and 3). The nuclear and extended family together were identified more often as primary sources of support than all non-familial support sources combined. Service members ranked spouses and friends highest among support personnel across SSQ subscales (Table 4).
Table 2Wilcoxon Signed-Rank Tests for highest-ranked support person for service members
| SSQ Subscale | |Z| | M (c, d) | a > b | p | |
| Nuclear vs extended/non-family | |||||
|
Dependable help (SSQ1) |
5.41 | 9, 8 | 67 > 8 | < 0.001*** | |
|
Really count on (SSQ2) |
5.14 | 9, 8 | 65 > 11 | < 0.001*** | |
|
Total acceptance (SSQ3) |
5.11 | 9, 8 | 67 > 8 | < 0.001*** | |
|
Really cares (SSQ4) |
6.36 | 9, 8 | 71 > 5 | < 0.001*** | |
|
When in dumps (SSQ5) |
5.60 | 9, 8 | 67 > 9 | < 0.001*** | |
|
When upset (SSQ6) |
6.42 | 9, 8 | 70 > 6 | <.001*** | |
| Nuclear/extended vs non-family | |||||
|
Dependable help (SSQ1) |
7.23 | 9, 6 | 74 > 1 | < 0.001*** | |
|
Really count on (SSQ2) |
6.32 | 9, 5 | 69 > 7 | < 0.001*** | |
|
Total acceptance (SSQ3) |
7.24 | 9, 1 | 72 > 3 | < 0.001*** | |
|
Really cares (SSQ4) |
7.65 | 9, 2 | 75 > 1 | < 0.001*** | |
|
When in dumps (SSQ5) |
6.73 | 9, 0.5 | 69 > 7 | < 0.001*** | |
|
When upset (SSQ6) |
7.30 | 9, 0 | 73 > 3 | < 0.001*** | |
Notes. *** p < 0.001
a Negative ranks
b Positive ranks
c Nuclear family median or nuclear/extended family median
d Extended/non-family median or non-family member (other) median
Table 3Wilcoxon Signed-Rank Tests for number of support persons for service members
| SSQ Subscale | |Z| | M (c, d) | a > b | p |
| Nuclear vs extended/non-family | ||||
|
Dependable help (SSQ1) |
7.10 | 1, 5 | 3 < 65 | < 0.001*** |
|
Really count on (SSQ2) |
3.79 | 1, 2 | 25 < 43 | < 0.001*** |
|
Total acceptance (SSQ3) |
6.09 | 1, 4 | 10 < 56 | < 0.001*** |
|
Really cares (SSQ4) |
6.15 | 1, 4 | 12 < 57 | < 0.001*** |
|
When in dumps (SSQ5) |
2.54 | 1, 2 | 29 < 33 | 0.011* |
|
When upset (SSQ6) |
2.68 | 1, 2 | 28 < 36 | 0.007** |
| Nuclear/extended vs non-family | ||||
|
Dependable help (SSQ1) |
5.34 | 4, 1 | 53 > 12 | < 0.001*** |
|
Really count on (SSQ2) |
4.75 | 2, 1 | 55 > 11 | < 0.001*** |
|
Total acceptance (SSQ3) |
6.36 | 4, 1 | 60 > 10 | < 0.001*** |
|
Really cares (SSQ4) |
7.04 | 4, 1 | 68 > 7 | < 0.001*** |
|
When in dumps (SSQ5) |
5.72 | 2.5, 0.5 | 61 > 8 | < 0.001*** |
|
When upset (SSQ6) |
5.85 | 2, 0 | 63 > 9 | < 0.001*** |
Notes. * p <.05, ** p <.01, *** p <.001, † trend at p <.10
a Negative ranks
b Positive ranks
c Nuclear family median or nuclear/extended family median
d Extended/non-family median or non-family member (other) median
Table 4Overall points and frequencies for top support person categories
| Spouse | Mother | Father | Children | Brother | Sister | Friends | |
| SSQ1 | 645 | 271 | 250 | 44 | 189 | 231 | 561 |
| Freq. | 73 | 41 | 36 | 8 | 30 | 28 | 114 |
| SSQ2 | 626 | 142 | 126 | 185 | 92 | 102 | 508 |
| Freq. | 71 | 23 | 20 | 28 | 14 | 22 | 83 |
| SSQ3 | 631 | 351 | 278 | 78 | 156 | 203 | 445 |
| Freq. | 71 | 50 | 39 | 28 | 24 | 38 | 86 |
| SSQ4 | 657 | 343 | 274 | 221 | 165 | 184 | 372 |
| Freq. | 74 | 50 | 40 | 18 | 27 | 39 | 80 |
| SSQ5 | 606 | 200 | 133 | 286 | 96 | 113 | 459 |
| Freq. | 68 | 29 | 21 | 45 | 15 | 22 | 83 |
| SSQ6 | 653 | 215 | 139 | 80 | 63 | 126 | 329 |
| Freq. | 73 | 30 | 21 | 5 | 9 | 26 | 59 |
| Total points | 3818 | 1522 | 1200 | 894 | 761 | 959 | 2674 |
| Total freq. | 430 | 223 | 177 | 132 | 119 | 175 | 505 |
Notes. Freq. = frequency each category was identified by service members
RQ 4: Leadership influence
Results demonstrated communication/check-ins, time off/family time, empowerment/encouragement, support, and providing information/resources as the highest-ranked effective leadership actions for the individual service members’ wellbeing (Table 5). Service members identified demanding behaviour, overwork, poor behaviour, lack of communication/check-ins and a lack of compassion as ineffective leadership actions for individual wellbeing. For family wellbeing, service members reported that effective actions by leaders included granting time off/family time, general support (e.g., moral and verbal), communication/check-ins, providing information/resources and household help. Ineffective actions by leadership related to family wellbeing included being overly demanding and/or overworking personnel (Table 5).
Table 5Highest-ranked themes in leadership support for service member wellbeing
| Theme | Freq. | Freq.% | Score | Score % | Quote | |
| Personal wellbeing | ||||||
| Effective | ||||||
| Communication/check-in | 26 | 17% | 60 | 17% | ‘Constantly checking in on me’ | |
| Time off/family time | 24 | 15% | 58 | 16% | ‘Provided time off’ | |
| Empowerment/encouragement | 22 | 14% | 53 | 15% | ‘Encouraged a team approach’ | |
| Support | 14 | 9% | 33 | 9% | ‘Moral support’ | |
| Providing Information/resources | 10 | 6% | 23 | 7% | ‘Help find support’ | |
|
Total for question
|
155 | 354 | ||||
| Ineffective | ||||||
| Demanding/overworked | 30 | 28% | 50 | 19% | ‘Placed more focus on military regulations than recovery’ | |
| Poor behaviour | 18 | 17% | 32 | 12% | ‘Verbal abuse’ | |
| Lack of communication/check-ins | 16 | 15% | 28 | 11% | ‘Poor communication with families during deployment’ | |
| Lack of compassion | 11 | 10% | 22 | 9% | ‘Business as usual approach’ | |
| None/no Answer | 9 | 8% | 32 | 12% | *Service members indicated no ineffective behaviours by leaders | |
|
Total for question
|
106 | 259 | ||||
| Familial wellbeing | ||||||
| Effective | ||||||
| Time off/family time | 30 | 22% | 82 | 26% | ‘Gave me more downtime’ | |
| Support | 18 | 13% | 41 | 13% | ‘Responded to needs while I was away’ | |
| Communication/check-In | 16 | 12% | 40 | 12% | ‘Periodic check in with family during deployment’ | |
| Providing Information/resources | 11 | 8% | 30 | 9% | ‘Making us aware of the opportunities available to us’ | |
| Household help | 9 | 7% | 21 | 7% | ‘Arranged transportation and living needs’ | |
|
Total for question
|
137 | 321 | ||||
| Ineffective | ||||||
| Demanding/overworked | 27 | 28% | 73 | 31% | ‘Not giving leave when needed’ | |
| Lack of compassion | 9 | 9% | 22 | 9% | ‘Failed to understand family needs’ | |
| Lack of information/resources | 7 | 7% | 18 | 8% | ‘Not pass on information’ | |
| Lack of communication/check-Ins | 6 | 6% | 12 | 5% | ‘No programs in place to support them’ | |
| None/no Answer | 13 | 14% | 36 | 15% | *Service members indicated no ineffective behaviours by leaders | |
|
Total for question
|
96 | 236 | ||||
Notes. Freq. = Count of response per thematic category. Freq. % = Percentage of freq. divided by total frequency for question. Score = Total ranked scores of responses. Score % = percentage of total ranked scores divided by total score for question. Top five categories were included for each theme out of 14-17 categories, dependent on theme.
Discussion
This study utilised validated instruments to explore support for service members based on the MFFM. Unit, community and social supports—as well as leadership influences—were specifically investigated as external resources for resilience post-deployment. The MFFM was partially supported in RQ1: unit support was not predictive of emotional wellbeing during deployment, but was predictive at post-deployment. RQ2, with community support, did not predict emotional wellbeing for service members and did not support the MFFM. RQ3 examines family support and RQ4 explores leaders’ impact on service members, highlighting their significant influence and serving as important external resources identified in the MFFM.
Unit support post-deployment was more impactful on emotional wellbeing than unit support during deployment, reflecting the stressful operational demands during deployment that limit psychological benefits of unit-based support. Conversely, post-deployment may often allow for greater reflection, interpersonal connection and the restoration of cohesion, enabling unit support to improve emotional resilience. The nuclear family emerged as the most significant source of social support. Spouses as the primary support for this married sample underscores these relationships. Past research, as this research does, suggests that unit support may bolster wellbeing6 and in this study, leaders may also impact wellbeing in a sample of more senior officers. Effective leadership communication promoted service member and family wellbeing. In contrast, ineffective leader support for wellbeing was most often identified as an imbalance between mission demands and the needs of service member and their family. The preliminary findings from this study on unit support, social support and leader influence establish a foundation of positive results for further investigation.
Limitations
The current study can be extended by using a more representative sample, adopting a more robust methodology and conducting further investigations into the measurement of the MFFM. The use of validated instruments that do not comprehensively measure the MFFM presents a limitation. For example, the DRRI Section L measure of community support does not capture the breadth of military and veteran service organisations’ resources, thereby preventing insights into the post-deployment support they offer. The convenient sample, though an underresearched group, overrepresents select service members (e.g., married, white, male officers; higher educated), preventing generalizability. Non-married service members were excluded, underscoring the need to understand the support systems parents and friends. Furthermore, delayed reporting of data collected between 2011 and 2013 is typical of military research due to information/operational security requirements and iterative rounds of qualitative and quantitative analyses. Despite these limitations, the lessons learned about resilience and wellbeing from this current study provide valuable insight, not previously reported.
Future research
Future research should expand participant recruitment to additional installations and locations to better represent the US military. Including service members from other geographic locations increases the likelihood that the sample will include participants who are currently underrepresented and better reflect the external resources required for the variety of experiences that military service presents. With an expanded sample, the measurement of the Military Family Fitness Model can be tested to comprehensively understand the influence of demands on service members’ adaptive outcomes.
Although time has passed since data collection, the issues addressed in this study remain relevant and should continue to be prioritised by the current US military. With anticipated Large-Scale Combat Operations (LSCO) in future wars,30 service members will benefit from innovative, validated solutions that directly improve unit cohesion and family support.
Conclusion
This preliminary study highlights the important role of unit and leader support in service members’ resilience and wellbeing post-deployment. The nuclear family (e.g., spouse and children) is a central support; however, extended family (e.g., parents and siblings) and friends also provide unique support to service members throughout deployment. Military policy and leadership training, as well as social support training, may further enhance the integration of family support into mission management, with a focus on long-term resilience and the wellbeing of service members.
Corresponding Author: Stephen V Bowles, stephen.bowles.ndu@gmail.com
Authors:
S Bowles1,2
D Hoffman3
F M Cozzi4
S Bujtor5
E Grieser6
S Kilar7
A P Siddall8
A Ghosh9
J E M Novosel-Lingat20
T Hoyt11
Author Affiliations:
1 Institute of National Strategic Studies, National Defense University
2 Uniformed Services University of the Health Sciences
3 Department of Psychology, Northern Illinois University
4 Cambridge Brain Tumour Imaging Laboratory, Division of Neurosurgery, Department of Clinical Neurosciences, Addenbrooke’s Hospital, University of Cambridge, Hills Road, Cambridge CB2 0QQ, United Kingdom
5 Florida State University
6 United States Air Force
7 University of Pennsylvania
8 Georgetown University
9 University of Kansas
10 Tripler Army Medical Center
11 Defense Health Agency, Medical Affairs Directorate
We would like to acknowledge Anna Goyette, Evan R. Hughes and Paul Switzer for their initial contributions to the paper.
The views expressed in this manuscript are those of the authors and do not reflect the official policy or position of National Defense University, Uniformed Services University of the Health Sciences, Defense Health Agency, United States Air Force, United States Army, United States Department of War, and the United States Government.
Please specify the URL of your file