
Abstract
Veterans are frequently exposed to chronic stress, trauma, moral injury and psychosocial risks that extend long beyond service. Traditional wellbeing interventions can overlook the spiritual and existential aspects of suffering. This study responds to a need for integrated pastoral innovations that strengthen veteran self-care and recovery by identifying psycho-spiritual mechanisms that complement self-compassion. While self-compassion is a recognised buffer for stress, evidence shows its effects are inconsistent when used alone, with chaplains frequently observing deeper needs related to meaning, identity repair and compassionate boundary-setting.
A Critical Interpretive Synthesis (CIS), supported by heuristic inquiry and bricolage, was used to integrate literature from pastoral care, positive psychology, spirituality, and workplace wellbeing within a biopsychosocial-spiritual (BPSS) framework. Findings suggest that self-compassion is enhanced when paired with humility, which is accurate, non-judgemental self-awareness and psycho-spiritual detachment, a tender, meaning-oriented ‘stepping back’ from rumination and self-criticism. These mechanisms appear to support healing, moral repair, emotion regulation and self-care. Chaplains can support these mechanisms through relational presence, narrative repair, ritual, reflective practices and collaboration with psychology. A conceptual pastoral framework and brief pastoral practice guide are presented to help embed inclusive spirituality, reflective practices, chaplaincy access and compassion-based initiatives into veteran support systems and organisational wellbeing frameworks.
Keywords: self-compassion, veteran stress, humility, psycho-spiritual detachment, chaplaincy
Introduction
Many military veterans and similarly, police and emergency service veterans, live with persistent stressors that do not end with discharge. Combat exposure, morally complex decisions, and the deaths of comrades are linked to long-term PTSD1, depression, suicidality and moral injury. When purpose, hope and spiritual frameworks become sources of guilt or collapse entirely, distress often intensifies.1 Conversely, positive spiritual coping and renewed meaning can buffer psychological strain and promote healing and recovery.
Many veterans, therefore, seek integrated psycho-spiritual care that combines mental health treatment with chaplaincy. Evidence shows high veteran engagement with chaplains for mental health concerns, but collaboration with clinicians often remains fragmented despite clear demand.2 Contemporary approaches increasingly recommend bio-psycho-social-spiritual (BPSS) models that embed chaplains within trauma and moral injury care pathways.
Veterans frequently report loss of meaning, hopelessness and identity disorientation, strongly related to PTSD symptoms, suicide risk and moral injury. These challenges are not only psychological but existential. Chaplains play a crucial role by offering relational, spiritually attuned presence, facilitating meaning-making, supporting rituals and linking veterans with appropriate services.
Context: The Biopsychosocial-Spiritual (BPSS) framework
Pastoral carers and chaplains work alongside clinical, psychological and social supports to address the full spectrum of veteran wellbeing. When individuals engage in negative self-talk or harsh inner criticism, they often experience spiritual degradation, loss of purpose and weakened hope. However, historically, many care frameworks have omitted religious or spiritual components, prompting the development of the BPSS framework to ensure spirituality and meaning-making are included.3 As Layson notes, models of moral distress such as moral injury and perceived injustice are best understood within a broader anthropological category of “moral suffering,” which the BPSS framework addresses by restoring spiritual and existential elements often neglected in organisational responses.2
Recent evidence suggests that work practices integrating psycho-spiritual and compassionate dimensions play a protective role in high-risk occupations. Martins, Palmeira and Matos demonstrate that spiritually informed practices can buffer the effects of stress. At the same time, Goff et al. found that organisational support for religion and spirituality reduced burnout even after controlling for personal religiosity and workplace support.5,6 These findings show that spirituality broadly defined contributes to resilience and psychological health.
Although chaplains offer confidential, relational, spiritually grounded care to those experiencing betrayal, which complements clinical services, research remains limited and sometimes methodologically fragmented.7 Chaplains often teach reflective practices such as mindfulness, self-kindness and perspective-taking. These practices align closely with the BPSS model because they recognise the interplay of psychological, relational and spiritual factors in recovery.
Self-compassion
Self-compassion is an important construct in veteran care, especially for individuals living with trauma-related guilt, stress, shame or moral conflict. Grounded in three components: self-kindness, common humanity and mindfulness.8 However, research consistently shows that self-compassion alone may not be sufficient. Its conceptualisation varies across studies, sometimes as a trait, sometimes as a skill, leading to mixed results.9
Research with veterans shows significant individual differences in responses to self-compassion practices, implying that other mechanisms influence outcomes. This supports the view that self-compassion is most effective when complemented by additional psycho-spiritual resources, a key premise of this study.
Aims and research question
Scholars increasingly emphasise the need to integrate spiritual and moral domains into biopsychosocial care.10 Military chaplains are often a first, a trusted contact for members experiencing shame, guilt, negative self-talk or meaning disruption.11 Emerging models show that spiritually integrated approaches to moral injury, combining chaplaincy with meaning-making, forgiveness and values repair, complement clinical treatment rather than duplicate it.12
The premise of this study is that self-compassion, while valuable, may be strengthened when paired with other psycho-spiritual mechanisms. The aim is to search for and synthesise such mechanisms, particularly those that support meaning-making, relational repair and emotional regulation. Findings may extend beyond military contexts to other trauma-exposed workplaces.
Research question
Noting that self-compassion fosters healing and resilience in veterans exposed to stress and moral injury, a key question is: what additional self-care choices could complement self-compassion, given the subjective and relational nature of pastoral care?
Method
The study adopts a Critical Interpretive Synthesis (CIS) approach. This is a theory-generating, interpretive method well suited to pastoral care’s psycho-spiritual, relational and moral dimensions. It resists narrow quantification.13 CIS enables iterative searching, appraisal and synthesis across diverse literatures while acknowledging disciplinary biases. The researcher plays an active interpretive role, reflecting the intuitive, experiential nature of pastoral practice.
Spirituality in this paper is defined broadly as ‘lifestyles and practices that embody a vision of human existence and how the human spirit achieves its potential’.14 This definition aligns with contemporary chaplaincy, where pastoral care addresses identity, belonging and meaning within psychological distress.
The CIS process involved systematic searches, critical appraisal of conceptual contributions, and development of thematic constructs. Heuristic and bricolage perspectives were incorporated to reflect the adaptive, interdisciplinary nature of psycho-spiritual care.15,16 Bricolage is relevant because pastoral carers routinely draw as many themes, mechanisms and disciplines as necessary in response to need.
To enhance the credibility, transparency and conceptual rigour of the synthesis, where possible, the analysis incorporated negative case analysis, a systematic strategy for identifying evidence that contradicts, complicates or challenges emergent interpretations. Rooted in traditions of qualitative rigour, this approach intentionally seeks studies, themes or data segments that deviate from dominant patterns, thereby testing the stability, scope and explanatory power of developing constructs. Within a Critical Interpretive Synthesis (CIS), negative case searching plays a crucial role in refining theoretical propositions by revealing potential over generalisations, exposing conceptual tensions and promoting deeper integrative thinking.13 Likewise, heuristic and bricolage-informed methodologies emphasise the importance of attending to disconfirming evidence as part of disciplined reflexivity, helping prevent premature closure around preferred interpretations.16
In this study, negative case analysis was applied iteratively: as themes such as self-compassion, humility or psycho-spiritual detachment consistently appeared to be supported, the review process deliberately sought empirical or conceptual counterexamples, including critiques of the Self-Compassion Scale, limitations of detachment and challenges to spirituality-based interventions. This procedure strengthened analytical depth, clarified the boundaries of applicability, and contributed to a more nuanced and trustworthy synthesis.
Literature review
This intuitive literature search focuses on veterans’ self-care and pastoral–chaplaincy practices that complement self-compassion and address the inner life. It also co-opts material from related disciplines. A key starting point is Litz et al.’s foundational work on moral injury, demonstrating how morally injurious events disrupt moral identity, purpose and meaning.17 Such events often produce guilt, shame, spiritual distress and long-term psychosocial impairment. Veterans may also experience spiritual/ religious struggles that paradoxically coexist with renewed faith or increased prayer as protective strategies.18
Self-compassion, which includes self-kindness, common humanity and mindful acceptance, is recognised as psychologically and spiritually grounded, supporting recovery from stress and trauma. Originating in contemplative traditions, self-compassion counters harsh self-criticism and guilt commonly found in trauma-exposed professions.8 Yet self-compassion sits within a broader field of workplace spirituality and meaning.
Work-related spirituality and meaning
Evidence shows that work-related spirituality reduces affective rumination and encourages constructive problem-solving.19 Emergency nurses and paramedics who use positive spiritual coping strategies report lower occupational stress, suggesting spirituality’s potential to serve as an emotional regulator in high-pressure roles.20 These studies affirm the value of meaning-oriented coping, yet they did not examine self-compassion.
Compassion-based interventions
Growing attention has been given to compassion-based interventions (CBIs) as methods to reduce stress and enhance wellbeing. It was found that CBIs promoting compassion, self-compassion and mindful reflection significantly lowered stress and improved emotional wellbeing across occupational groups.5 Then other research demonstrated that brief workplace compassion-focused training reduced perceived stress and burnout while increasing self-compassion and work engagement.21
While some studies report only modest reductions in depression or variability in outcomes, CBIs generally support employees’ emotional regulation and meaning-making.5 Organisational support and psychological safety are key moderators.22 Research also shows that loving-kindness and compassion meditation support workplace wellbeing.23 These suggest that compassion practices can be spiritual, psychological and organisationally influenced.
Self-compassion and its limitations
Evidence shows that self-compassion buffers the adverse effects of poor psychological detachment, reducing emotional exhaustion and depressive symptoms.24 Therefore, self-compassion has become an increasingly important aspect of veteran care, especially for individuals living with trauma-related guilt, shame or moral conflict. It is centred around three components: self-kindness, common humanity and mindfulness.8
Self-compassion helps veterans relate to their suffering with warmth rather than harsh judgement. Studies show that higher levels of self-compassion predict fewer PTSD symptoms and support more stable recovery trajectories, even when combat exposure is high.25 These findings highlight the central role of how veterans relate internally to their distress.
However, research consistently shows that self-compassion alone may not be sufficient. Its conceptualisation varies across studies, sometimes as a trait, sometimes as a skill, leading to mixed results.9 Some interventions show modest or no greater impact than general reflective writing, suggesting that broader psycho-spiritual or reflective processes may be responsible for improvements.26 Questions have also been raised about the psychometric clarity of the Self-Compassion Scale, which may conflate self-criticism with low self-compassion.27
Further, physiological research with veterans shows significant individual differences in responses to self-compassion practices, implying that other mechanisms influence outcomes. This supports the view that self-compassion is most effective when complemented by additional psycho-spiritual resources: a key premise of this study.
Self-compassion training reduces burnout, with some studies showing benefits for deeper trauma, though results vary and other factors appear influential.28 Detachment itself is not always effective, especially when positive moods or meaning-oriented reflections are more appropriate.29 This suggests that self-compassion and psychological detachment, while useful, are insufficient by themselves.
Role identity also shapes outcomes. Individuals with strong callings (clergy, chaplains, health professionals, military personnel) often struggle to detach from work, experiencing ongoing responsibility beyond the shift.30 Even though detachment is generally beneficial, meta-analytic evidence shows that job characteristics and personal values shape its effects.31
Self-compassion moderates emotional exhaustion, but multidimensional approaches can offer more durable protection.24 For chaplains, self-compassion relates to positive psychology and appears protective in moral injury recovery by promoting kindness and acceptance in the face of distressing events.32 It also counteracts shame and guilt in moral injury.
Longitudinal studies further show that self-compassion supports adjustment, emotional functioning and quality of life. An 8-week Mindful Self-Compassion program for morally injured veterans yielded reductions in PTSD symptoms, shame and distress, alongside increases in self-compassion.33 Similarly, integrating Acceptance and Commitment Therapy (ACT) with self-compassion helps strengthen psychological flexibility while ensuring self-kindness.8,34
Negative case analysis: self-compassion
While self-compassion is widely associated with improved wellbeing and reduced stress in workplace settings, negative case analysis highlighted several studies that complicate this narrative. Some evidence suggests that self-compassion may not uniformly benefit all workers; in certain contexts, it can blur with self-criticism or fail to buffer stress as strongly as proposed.9 Other research indicates, not surprisingly, that self-kindness alone has a positive effect, suggesting that the ways the three aspects of self-compassion work as a construct need closer examination.35
Research also shows that self-compassion does not necessarily improve problem-solving, nor does it consistently outperform other mechanisms such as meaning-making or reflection.36,37 Psychometric critiques argue that the Self-Compassion Scale may blur distinctions between self-compassion and self-criticism.35,38 Understanding the research immediately above enables a more nuanced understanding of self-compassion’s effect and operations, or lack thereof on occasions, emphasising that its impact may vary by other factors, including individual personality factors and the presence of complementary supports, such as meaning-making or humility practices. Overall, however, evidence supports self-compassion as valuable but incomplete unless paired with other reflective, spiritual or relational mechanisms.
Other mechanisms: meaning-making, reflection, forgiveness
Meaning-making emerges as a consistent buffer for stress and moderates the relation between work stress and life meaning.39 Jnaneswar and Sulphey demonstrated that workplace spirituality, mindfulness, and self-compassion jointly predict mental wellbeing, indicating that combinations of responses, rather than single strategies, are most effective.40 Other research similarly found that self-compassion and reflection reduce psychological distress.41 Forgiveness also reduces stress by processing anger and resentment, fostering emotional healing.42 Spiritual practices such as empathy, prayer and positive self-talk support forgiveness, especially among religious or spiritually oriented individuals.43
Recovery skills that incorporate meaning-making, detachment, gratitude and positive rumination show associations with lower distress.44 Positive or constructive rumination can also have purposeful outcomes.45
Reflection has further relevance. Mamede and Schmidt identified five elements of reflective practice: deliberate induction, deduction, synthesis, openness to reflection and meta-reasoning.46 These processes promote thoughtful responses under stress and may reduce cognitive load in complex situations. New pastoral frameworks, therefore, need to support reflective practices, updated thinking and balanced responses to distress.47
Converging themes
The literature suggests that the limitations of self-compassion in isolation call for additional, personal and psycho-spiritual self-care choices. Two mechanisms emerge strongly: humility and psycho-spiritual detachment. Both relate to accurate self-view, self-kindness, reduced harsh self-talk and sustained meaning-making. Together with self-compassion, they offer integrated pathways to coping, identity repair and reduced burnout.
Discussion
Research shows that meaning-making and inner spiritual work can support stress reduction and modest improvements in PTSD symptoms among veterans. It was demonstrated that post-deployment meaning-making, asking ‘Who am I now?’ and ‘How do I live a good life?’, influences whether moral and spiritual injuries remain sources of distress or become integrated into a coherent life narrative.48 This meaning-making functions as an existential ‘stepping back’, enabling veterans to observe traumatic experiences with greater psychological spaciousness.
Structured interventions likewise reveal the significance of meaning. For example, a Search for Meaning group, an eight-session spiritually based program, produced statistically significant reductions in PTSD symptoms, spiritual injury, and negative religious coping among veterans, indicating that guided work on purpose and belief systems can reduce suffering and enhance emotional regulation.49
Similarly, it was found that veterans’ treatment outcomes were shaped by religiosity, spirituality and especially a sense of purpose.50 These findings show that meaning-making acts both as a buffer and a form of psycho-spiritual grounding, helping veterans live alongside trauma without being continually overwhelmed. Taken together, the literature suggests that psycho-spiritual detachment in veterans often works through meaning: establishing a stable narrative or purpose that allows trauma to be held rather than avoided.
Psycho-spiritual detachment
In the context of workplace stress, psycho-spiritual detachment—also called meaningful or spiritual detachment—is defined as a gentle, self-caring process of ‘letting go’ of unhelpful rumination, inner criticism and persistent stress-related emotions.51 It reflects a spiritually grounded form of non-attachment that enables individuals to step back from moral pain and evaluate experiences with compassion and perspective.
Emerging research on moral injury shows that spiritually informed practices, including confession, forgiveness rituals and spiritual surrender, can reduce guilt, shame and PTSD symptoms in military populations.52,53 These practices often engage the same reflective, meaning-oriented stance central to psycho-spiritual detachment.
Psychological detachment itself involves non-judgemental awareness of one’s inner experience51 and aligns with mindfulness-based coping.8 Unlike emotional withdrawal, psycho-spiritual detachment is tender, self-protective, and relational, creating space for inner quietness, reflection and emotional integration. It complements self-compassion by reducing over-identification with distress and encouraging kinder, more balanced self-observation.
Validated measures such as the Recovery Experience Questionnaire29 and detachment indices can assist assessment, though spiritual aspects often require heuristic interpretation.54
Psycho-spiritual detachment is therefore not passive disengagement. It combines the following, which make it relevant for veterans processing moral injury, cumulative stress, and identity disruption:
- inner spaciousness
- perspective-taking
- reduced rumination
- emotional openness
- acceptance of imperfection.
These features make it highly relevant for veterans processing moral injury, cumulative stress and identity disruption.
Humility
Humility is defined as accurate self-awareness, openness and a non-dominating presence; these qualities emerge as another key complementary mechanism. Humility supports self-kindness by encouraging individuals to acknowledge limitations without shame and to extend compassion to themselves during adversity.55
Evidence is growing that humility protects against emotional disturbance in trauma-exposed populations. Veterans with higher humility-related traits report fewer post-traumatic reactions and reduced emotional volatility.56,57 In the moral injury literature, humility-related processes such as forgiveness, self-forgiveness and the acknowledgment of limits are frequently presented as conditions for recovery. Veterans often describe forgiveness as ‘opening a door’, signalling reduced guilt and reconnection with self and community.20
Humility also fosters psychological safety, essential for team cohesion, help-seeking and compassionate communication.58,59 However, this has not been studied much with veterans. Irrespective, others highlight that humility promotes adaptability, emotional regulation and openness to new perspectives.60 The strongest benefits of humility are relational, expressed through altruism, empathy, forgiveness, cooperation and self-control.
Humility can be modelled and taught. Research shows that leader-expressed humility reduces stigma and encourages help-seeking.61,63 The Comprehensive Intellectual Humility Scale57 provides a validated measure of this virtue.
Importantly, humility is not self-abasement. It is a realistic acceptance of one’s strengths and limitations that supports non-judgemental self-view and reduces harsh self-criticism—making it a natural complement to self-compassion. When combined with psycho-spiritual detachment, humility helps individuals maintain boundaries, reduce rumination and approach suffering with tenderness and clarity rather than defensiveness.
The three complementary mechanisms
Across the literature, three themes appear to relate to meaningful self-care, to one another and even overlap. These are as follows and illustrated below in Figure 1:
- Self-compassion: warm, mindful, non-judgemental self-awareness
- Psycho-spiritual detachment: tender, meaning-oriented emotional stepping back
- Humility: accurate self-view, openness and acceptance of imperfection

Figure 1: Overlapping self-care themes/choices in support of meaningful self-care
Together, they support the following and form the conceptual basis for the framework developed later in the manuscript:
- reduced self-criticism
- improved emotional regulation
- healthier boundaries
- moral and spiritual repair
- resilience in high-stress contexts.
Chaplaincy and organisational context
Chaplains play an important role in supporting self-care actions through pastoral presence, helping individuals step back meaningfully from distress and cultivate accurate, compassionate self-views. They often triage moral and emotional concerns, assist veterans in reconnecting with meaning, and foster tender detachment from trauma through spiritually informed practices such as deep listening, values clarification, ritual, lament and reflection.64 Chaplains help restore boundaries, dignity and emotional clarity while activating referrals to clinical, psychological and peer supports when required.
This relational, spiritually attuned presence complements psychological care. Chaplains often work at the interface of ethics, identity, purpose and trauma domains central to moral injury. By helping individuals narrate, process and situate difficult experiences within broader value and belief systems, chaplains facilitate important shifts in trust, self-compassion and moral orientation.
Organisational factors and psychosocial safety
Chaplaincy most often operates within organisational contexts, for example, Veterans Administration, which are shaped by psychosocial safety, leadership behaviours, workload demands and support structures. These factors influence both wellbeing and the effectiveness of pastoral care.65 In this environment, chaplains frequently co-work with psychologists, peer support officers, health staff and leaders, contributing to workplace culture, moral repair and psychological safety.
Contemporary models of pastoral innovation emphasise integration with organisational wellbeing strategies, particularly those aligned with ISO 45003 psychosocial risk frameworks.
Compassion-based training, reflective practices and spirituality-informed initiatives can be embedded as proactive risk controls rather than optional add-ons.42,66 When such supports are legitimised in policy and culture, they promote emotional regulation, purpose, connection and trust.
Arguably, compassion is not merely a personal virtue but an organisational capability.5 When leaders model compassion, and when workplaces normalise reflective practices and access to chaplaincy, employees experience deeper support, better recovery and improved relational climates. Spirituality, wellbeing initiatives and meaning-making become embedded in organisational life rather than peripheral.
This aligns with the BPSS framework, which views organisational, relational and individual wellbeing are interconnected. From a pastoral perspective, humility, tender detachment and self-compassion become not only personal mechanisms but cultural resources that strengthen collective resilience.
Transition to conceptual framework
Drawing on the CIS synthesis, three complementary self-care mechanisms are self-compassion, humility and psycho-spiritual detachment. emerged as central pathways to supporting veterans experiencing moral injury, trauma and chronic stress. These mechanisms work best when supported by chaplaincy practices that include narrative repair, meaning-making and spiritually grounded reflection. Together, they are also encapsulated in a conceptual framework illustrated below. It shows how these three mechanisms operate at:
- individual levels (inner emotional regulation, reduced self-criticism, meaning reconstruction)
- relational levels (trust, connection, psychological safety)
- organisational levels (culture, leadership, psychosocial systems).
New conceptual framework
The conceptual map integrates the complementary mechanisms with chaplaincy practices and potential outcomes, forming the foundation for the pastoral practice guide. Using the biopsychosocial-spiritual (BPSS) lens, the CIS synthesis identified three interconnected psycho-spiritual self-care mechanisms: self-compassion, meaningful (psycho-spiritual) detachment and humility, as particularly salient in supporting veterans experiencing moral injury, trauma and prolonged stress. These mechanisms complement each other and collectively enhance psychological safety, meaning, self-care and relational trust.
1. Self-compassion
Self-compassion provides non-judgemental, emotionally balanced awareness of suffering. It helps counteract harsh self-talk, shame and guilt—common responses to moral injury—and encourages practical self-care choices grounded in kindness and shared humanity.67 In pastoral care contexts, self-compassion is integral to how individuals process trauma and re-engage with values.
2. Psycho-spiritual detachment
Psycho-spiritual detachment (or meaningful detachment) offers veterans a gentle, reflective ‘stepping back’ from distressing thoughts and emotions. It reduces over-identification with trauma, softens negative rumination and encourages spacious emotional processing.48 Detachment functions as a stabilising, meaning-oriented mechanism that restores perspective, supports spiritual grounding and allows values-based reorientation.
3. Humility
Humility enables accurate self-assessment and the acceptance of human limitations, countering perfectionism and self-condemnation—factors often heightened in moral injury and trauma. Humility fosters compassion, psychological safety and relational trust.52,55 It supports emotional regulation, openness and willingness to seek help, making it a powerful complement to self-compassion.
Pastoral Action Concept Map
The Pastoral Action Concept Map below in Figure 2 illustrates the relationship between self-compassion, meaningful detachment and humility, even to the extent that they can overlap:
- Self-compassion provides warmth and non-judgemental awareness
- Detachment creates emotional space to observe suffering without becoming overwhelmed
- Humility grounds the process with realism, acceptance and relational openness
Together, they form a model of spiritually grounded self-care:
- Emotional regulation (reducing rumination and harsh self-talk)
- Identity and moral repair (reframing beliefs, restoring dignity, reconnecting with values)
- Boundaries and resilience (establishing kinder internal dialogue, facilitating rest, reducing overload)
- Psychosocial safety and connection (fostering trust in teams, leaders and carers)
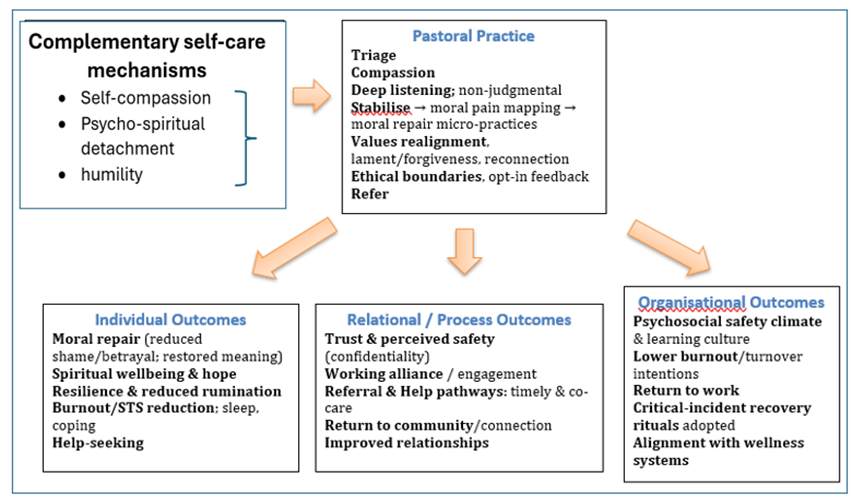
Figure 2: Pastoral Action Concept Map: self-care enablers, practices and outcomes
This model shows how pastoral care becomes a strategic element of veteran self-care and resilience. They are enablers, not merely a supportive resource but a core component of veteran wellbeing systems. These enablers prepare individuals for deeper emotional processing, boundary-setting, moral repair and sustained wellbeing.
It is important to acknowledge that the Pastoral Action Concept Map and (brief) Pragmatic Playbook proposed in this paper remain theoretical in their current form. Rather than presenting a validated clinical protocol, this paper offers a conceptual framework intended to synthesise existing evidence and translate it into a coherent pathway for veteran care. As such, it is offered as a starting point for dialogue rather than a prescriptive model. The authors therefore invite practitioner feedback, from clinicians, chaplains, mental health professionals and veterans themselves, as an essential next step in refining and contextualising this framework for real-world implementation. Such feedback will be critical in identifying practical barriers, cultural considerations and setting-specific adaptations that no theoretical model can fully anticipate in advance.
Chaplains are well positioned to activate and support these processes either with or without the map, through relational presence, value reflection, narrative repair, ritual, forgiveness work and integrated referral pathways.
A. Self-care enablers
- Self-compassion
- Meaningful/psycho-spiritual detachment
- Humility
- Reflective practice (meta-reasoning, narrative review)
- Spiritual awareness and values alignment
B. Pastoral practices
Pastoral and chaplaincy practices that activate and support these enablers include:
- deep, compassionate listening
- narrative repair and reflective dialogue
- rituals of lament, forgiveness and purpose
- meaning-making conversations
- boundary support and detachment cues
- referrals to psychological or medical care when indicated
- confidential relational presence
- psycho-spiritual education (values clarification, self-kindness, tender detachment).
Pastoral practices link the enablers to concrete behavioural and emotional shifts.
C. Individual outcomes
Examples include:
- reduced rumination
- improved emotional regulation
- enhanced meaning and identity coherence
- reduced guilt and shame
- greater self-kindness
- improved capacity to rest, detach and set boundaries
D. Relational outcomes
- Renewed trust
- Improved communication
- Reduced stigma
- Increased help-seeking
- Reconnection with partners, colleagues or community.
E. Organisational outcomes
- Enhanced psychosocial safety climate
- Stronger team cohesion and moral alignment
- Reduced burnout and compassion fatigue
- Improved wellbeing KPIs
- More integrated care pathways (psychology, chaplaincy, leadership).
Limitations
This synthesis is shaped by the interpretive nature of Critical Interpretive Synthesis (CIS), which involves researcher judgement and therefore carries risks of subjectivity and reflexivity bias. While such interpretive methods are appropriate for spiritual, relational and moral domains that resist reductionist measurement, the flexibility of CIS also limits replicability compared to traditional systematic reviews. The scarcity of contemporary chaplaincy research on self-compassion, humility and psycho-spiritual detachment further constrains the available evidence for integration—a limitation reflective of the field itself.
Many studies in the reviewed literature rely on cross-sectional or qualitative designs, limiting the capacity to infer causality. Heuristic and bricolage approaches enrich understanding but contribute additional subjectivity.15 Longitudinal evaluations of chaplaincy impact, particularly across deployments or entire careers, remain limited. There is also relatively little research examining how humility, detachment and self-compassion interact synergistically in workplace or military contexts.
While the findings offer promising conceptual insights, they require empirical testing to validate the proposed relationships among self-compassion, humility, psycho-spiritual detachment and chaplaincy practice.
Future research
Significant gaps exist in chaplaincy research and occupational wellbeing regarding psycho-spiritual self-care.68 Future studies should adopt mixed-methods designs that integrate qualitative insights with quantitative indicators, using outcome tools (e.g., moral injury scales, spiritual wellbeing measures, burnout indices) alongside narrative journals, reflective interviews and chaplain logs.69 Future research directions include:
- longitudinal research exploring the durability of humility, detachment and self-compassion as protective mechanisms
- intervention trials examining chaplain-led or co-delivered programs integrating mindfulness, compassionate reflection, forgiveness practices and meaning-making
- organisational studies assessing how psychosocial safety climates and leadership humility influence chaplaincy effectiveness
- interdisciplinary collaboration, such as the VA’s MHICS training and the integration of psychological modalities with spiritually grounded care
- evaluation of chaplain wellbeing examining how humility, detachment and self-compassion may reduce chaplain burnout, compassion fatigue and moral distress.51,67
Greater attention to humility and psycho-spiritual detachment, a still under-researched concept, may yield new insights into how spiritual care contributes to recovery, identity repair and resilience in trauma-exposed populations.
Summary and conclusion
The study began with the premise that self-compassion, while valuable for veterans experiencing chronic stress, trauma and moral injury, may be insufficient on its own. Using a CIS enriched by heuristic and bricolage perspectives, the research integrated literature across chaplaincy, positive psychology, pastoral care, spirituality and organisational wellbeing within a biopsychosocial-spiritual (BPSS) framework.
Self-compassion remains a crucial component of emotional resilience, helping veterans respond to distress with kindness rather than harsh self-judgement.8 However, two additional psycho-spiritual mechanisms emerged as consistent complements:
Psycho-spiritual (meaningful) detachment
This is a tender, reflective, emotional stepping back that reduces rumination, supports perspective and enables trauma to be held rather than re-lived.51,55 Such meaningful detachment helps individuals create inner space to process suffering without avoidance or denial.
Humility
Humility is an accurate, accepting self-view that reduces defensiveness, supports emotional openness and facilitates forgiveness, moral repair and willingness to seek help. Humility fosters relational trust and psychosocial safety while reinforcing self-compassion.47
Together, these three mechanisms form a spiritually grounded, evidence-informed triad of self-care that addresses both emotional and moral–existential domains of suffering. Each mechanism reinforces the others:
- Self-compassion softens suffering
- Detachment creates space around suffering
- Humility grounds suffering in acceptance, connection and realism
Chaplains are situated to operationalise this triad through relational presence, narrative repair, ritual, reflective guidance and collaborative care pathways. Their work supports identity reconstruction, meaning-making, emotional equilibrium and connection back to community and purpose.
The conceptual ‘Pastoral Action Concept Map’ and accompanying pragmatic playbook translate these insights into practice, offering a multilayered model across individual, relational and organisational domains. This approach situates chaplaincy not merely as support, but as a core element of psychosocial safety and organisational wellbeing.
This paper shows, at least at the conceptual level, that a shift towards spiritually inclusive, compassion-based and meaning-oriented care, embedded structurally within veteran services and wellbeing systems, can significantly reduce distress, strengthen resilience and promote holistic healing for those who serve.
Appendix
Self-compassion-oriented care: Chaplaincy for stress & moral injury:
a (brief) pragmatic playbook
1) Quick-start: what matters in your first 24–48 hours
Your posture: be present, open, humble, boundaried, trustworthy.
Your aim: stabilise, protect dignity, be kind to self and connect to supports.
Your guardrails: confidentiality (within policy), ‘do no harm’, informed consent,
opt-in. Constantly check with other mental health professionals
Rapid contact checklist (10–15 minutes)
- Respecting privacy and boundaries, make contact where they are (parade ground, station, patrol room, mess, family setting).
- Micro-grounding (60–90 sec): ‘Feet on the floor, slow breath in… out. Right now, you’re safe with me.’
- Name the moral or distress signal (guilt, shame, betrayal, moral confusion, grief, anger).
- Normalise + permission: ‘Many in your role feel this; you don’t have to carry it alone.’
- Confidentiality script (adapt locally): ‘I’m here as your chaplain. Our conversation is confidential, except for immediate risk to life or mandated reporting. I don’t write performance reports, nor tell your team or team leader. This space is for you.’
- Triage decision: Immediate risk? If yes → activate emergency protocol; if no/unsure → continue chaplaincy care pathway while seeking help, advice and assistance.
2) Core pathway for moral injury & high moral stress
- Purpose: offer a repeatable, humane sequence blending pastoral care, light-touch measurement and collaboration.
Step A – Stabilise & locate the wound (15–30 min)
- Containment: posture, breath, quiet room; ‘We’ll take this slowly.’
- Name the moral pain: ‘What value feels violated? Whose trust feels broken?’
- Offer solidarity, not solutions: ‘You’re not broken; you’ve been hurt in a moral way.’
Step B – Screen & choose a lane (5–10 min)
Use brief, acceptable tools (select one per domain; keep it light):
- Moral injury exposure/symptoms: brief items from MIES / MISS-M(SF) / MIOS
- Spiritual wellbeing: FACIT-Sp-12 short
- General distress (if needed): DASS-21 short
- Alliance/process: one Working Alliance item (‘Do you feel this time is helpful?’)
Decision lanes:
- Lane 1 – Watchful waiting + Pastoral care: mild burden; schedule follow-up
- Lane 2 – Chaplain-led moral repair: moderate MI load; offer Pastoral Narrative Disclosure (PND) elements, lament/forgiveness ritual, meaning-mapping, values repair
- Lane 3 – Co-facilitation / referral: severe symptoms or safety issues; coordinate with psychology/GP/peer support; remain spiritually present
Step C – Moral repair micro-practices (15–40 min)
- Narrative repair: invite the story, pace the hardest parts, mark turning points
- Lament & acknowledgement: ‘What needs naming out loud?’ (ritual optional: candle, coin, soil, scripture/prayer/poem)
- Realignment: surface core values; one small act to realign life with values this week
- Forgiveness work (when appropriate): responsibility, remorse, repair, release—never rush it
- Community re-link: partner, family, trusted colleague, faith group, veteran peer group
Step D – Close & plan (5–10 min)
- Self-compassion practice (60–120 sec): hand on chest, slow breath, phrase: ‘This is painful. Others at work know this pain. May I be kind to myself & do what’s wise next.’
- Psycho-spiritual/meaningful detachment and humility for next shift: Stop ritual at gate; Body reset (walk, shower); Re-entry intention (who/what matters after work)
- Humility: in conjunction with self-compassion, recognise we are all human and get stressed
- Book the next contact and, with consent, note a tiny outcome marker (e.g., slept 5 hours, told partner, attended ritual)
3) Micro-skills that lift effectiveness
Humility (relational safety amplifier)
- Behaviours: ask before advising; honour each other;’ wisdom; admit your limits and then co-opt others (to build teamwork); invite collaboration
- Phrases: ‘You’re the expert on your experience; I can walk with you.’ / ‘If this doesn’t help, tell me and we’ll try something else.’
Meaningful detachment (boundary keeping with warmth)
‘We must take the risk of legitimate attachment (fully feeling the emotion), learn its important message, and then have the presence and purpose to detach from that fascinating emotion after it has done its work. This is the gift and power of an emotionally mature person’. Richard Rohr
- Behaviours: empathic presence + clear edges; time-bound sessions; deliberate handover when risk rises
- Phrases: ‘I’m with you in this, and I’ll also help you connect with X for the parts outside my lane.’ / ‘Let’s hold the story here for today; we’ll pick it up safely next time.’
Self-compassion (burnout buffer & modelling tool)
- Daily 3-minute reset: breathe, name a stressor, offer kind words, choose a wise next step
- After-care for you (post-critical event): peer check-in, brief reflection notes, hydrating/food, movement, sleep target, micro-Sabbath. Seek regular supervision
4) Working with the system (PSC) so chaplaincy can actually work
- Brief leadership (10 minutes): top three moral stressors; one practice helping; one barrier command can remove; ask for one Psychosocial Safety Climate (PSC) action this month
- Integrate, don’t compete monthly touchpoint with peer support, psychology, welfare, etc
- Protect confidentiality: reaffirm in every commander changeover and incident review
5) Documentation & evaluation without killing the soul of the work – ethical, light-touch
- Log (de-identified where possible): contacts, themes, lane chosen, brief outcome at follow-up, referrals, rituals
- Avoid logging identifying moral content without consent
- Use delayed, opt-in feedback (2–6 weeks) with a one-item pulse (‘Did chaplain support help you move one step towards what matters?’)
A minimalist measurement bundle (pick 2–3)
- MI focus: brief items adapted from MIOS or MISS-M(SF) (local approvals)
- Spiritual wellbeing: FACIT-Sp-12 short
- Burnout/STS: ProQOL-5
- Alliance/process: 1–2 Working Alliance items
6) Longer term care (7–30 days)
- Narrative & ritual: embed a simple lament/meaning ritual after hard calls; co-design language; train two peer champions; success = officers ask for it next time
- Detachment at the Gate: end-of-shift 3-minute protocol; cue card at locker; success = earlier switch-off reports
- Chaplain + Psych 2-hander: 4–6 session MI group; agenda: values, lament, forgiveness, reconnection; closing ritual; success = shame reduction, renewed belonging
7) Personal sustainability for chaplains (non-negotiables)
- Regular supervision (spiritual/clinical)
- Peer round (15 min) after tough call: ‘What I noticed / carried / am setting down.’
- Borders: fixed off-duty windows; say ‘not now—tomorrow 0900?’ and keep it
- Three anchors: movement, presence/prayer/quiet, friendship
- Red flags: persistent cynicism, sleep collapse, secrecy about coping. escalate
8) One-page scripts & prompts
- Opening: ‘What’s the part of this that hurts most to remember?’ / ‘If a trusted mate had lived this, what would you say to them?’
- Values repair: ‘Which value got bent or broken—loyalty, fairness, duty, care, truth?’ / ‘Name one small act this week that honours that value.’
- Forgiveness (when appropriate): ‘Is there anything to ask or offer in forgiveness—towards yourself, another, God?’ / ‘What would repair look like, even one small step?’
- Close: ‘Between now and our next chat, what would kindness to yourself look like?’ / ‘Who could safely walk with you for the next few days?’
9) Rapid Chaplaincy Pathway (flow chart) – see attached
Print and place in notebook or duty folder
10) Leader briefing card (for commander ‘catch-ups’)
Biography
Rev. Professor Peter Devenish‑Meares is a chaplain, director and an interdisciplinary scholar‑practitioner whose decades of service span Defence, police chaplaincy, banking, community care, board leadership and higher education. He integrates pastoral care, organisational ethics, and trauma‑informed practice to shape compassionate pastoral leadership, advance applied research, and strengthen governance across diverse Australian institutions. He has chaired a large housing charity and St John Ambulance (Qld)
Corresponding Author: Professor Peter Devenish-Meares, devenip@hotmail.com
Authors: P Devenish-Meares1
Author Affiliations:
1 University of Southern QLD



