
Mr Chairman.
As the last Director General of Naval Health Services and now a member of the RANR (a component of the ‘part-time force’ of the Navy and the ADF), I welcome this opportunity to address you today.
In particular, I applaud the stated aims of this conference, which are to enhance knowledge about service life in the context of applying evidence-based medicine to assist the assessment of claims submitted by Veterans for benefits, and to most efficiently direct resources to future research.
The allotted time allows me only to skim the surface of this important topic. In doing so, I intend to present data to support my conclusions that:
-
- there is a very large repository of health-related information available in each of the Services, (particularly the Navy), the utility of which is devalued by the lack of resources that would allow continuing structured analysis;
- Navy has been well served by its Operational Health Support and its Occupational Health & Safety policies developed over the years as evinced by low morbidity and mortality figures despite frequently operating in highly dangerous environments; and
vigilance is needed to ensure that this state of affairs is maintained for the Fleet of the 21st century.
I propose to give firstly an overview of the range of data that is available for analysis, then some results that have been able to be readily accessed, and finally an insight into some of the problems faced by our men and women at sea as the RAN enters the 21st century.
Naval health records in peace and war
All three Services currently maintain extensive health records of both permanent and Reserve force members. In the case of the permanent force, these records are held in duplicate although this situation is currently under active review.
In the Navy, additional medical documentation has been maintained in the form of the Ship’s Medical Journal or Medical Log. These medical journals have been maintained in both war and peace since the commissioning of the first fleet in 1911. In keeping with Naval tradition, shore establishments are run as “ships”, and the naval sick-quarters and hospitals have also maintained their own medical journals and medical logs. Copies of all of these are held by the Naval Records section of the Office of Surgeon General, or in archives in Canberra.
For those of you who have the time, I commend to you the journal of one of my predecessors, Fleet Surgeon Darby, the senior medical officer of HMAS Sydney I. This journal is maintained in the archives of this building.
In his commissioning voyage from Scotland via Cape Town, Darby documents in considerable detail the treatment of venereal disease and Phthisis, and the clinical courses of ‘toxic pneumonia’ and acute onset diabetes mellitus. 2 In the absence of antibiotics and insulin, burial at sea was the outcome of these latter two cases.
Later in 1915, his account of the injuries and subsequent management of the surviving RAN and German wounded in the action with SMS Emden off Cocos Island makes compelling reading.
This of course reminds me that the period chosen for today’s discussion has largely excluded wartime operations with the possible exceptions of the Persian Gulf and Somalia. To state the obvious, the dangers posed by actual combat operations will generally be much greater than in training and in peacekeeping deployments. That is not to say that these latter type of operations are not challenging, and indeed Colonel Peter Warfe has provided a good account of the complexities of such operations as a result of his experience in Rwanda. 3
It is also fitting to remember that not all casualties occur as the result of enemy action.
The USAF F4 Sparrow missile attack on HMAS Hobart (DDG 38) in the Gulf of Tonkin in 1968 that resulted in two RAN fatalities and 8 to 10 injuries demonstrates how the fog of war can result in losses through ‘friendly free’. There have of course been many other examples of this including those sustained by our allies in Operation Desert Storm.
However the brief today is to cover health threats to Navy personnel since the Vietnam War.
Health of the Navy 1998
For the five years from 1987 to 1991, the Navy MEDREX computer-based system coded every consultation and medical classification board using the then ICD classification system. However the requirement to input data was manpower-intensive and it was down graded for this reason. During these five years, “Health of the Navy” statistics were produced on a six-monthly basis and gave some broad indication of the state of medical readiness of the personnel in the Navy, and also some crude morbidity data. In reality, it was infrequently accessed, and in hindsight, was underutilised and undervalued.
The passage of the Occupational Health and Safety (Commonwealth Employment) Act in 1991 has meant that from 1993 onwards, the ADF has captured statistics regarding all deaths both work-related and non-work related and most of the work-related illnesses and injuries. Utilisation of this data will undoubtedly have an impact on ADF operations in the future as the true costs are identified, and responsibility for payment passed back to the operational commanders.
The statistics that I present today, therefore, are confined to basic mortality, injury and invalidity data, relating mostly to this decade
Mortality
In the four-year period 1994 – 97, the Directorate of Defence Occupational Health and Safety recorded 22 deaths in serving RAN personnel. 6 Of these 22, if travel-related accidents are excluded, only two were attributed to service-related activities.
The first case was that of the Naval Pilot killed in the helicopter winch training accident at HMAS Albatross just prior to Christmas in 1995.
The second death, which is less clearly work-related, involved that of a 41-year-old senior sailor at HMA Stirling from secondaries from a malignant melanoma. When MEDREX maintained its registry for neoplastic disease, skin cancers, including melanoma, were the most frequently encountered forms of cancer. Protection for all ADF personnel from ultraviolet radiation in sunlight is now dictated by DI(G) PERS 16-10 (1996). However, it would be appropriate to acknowledge the early initiatives in the field of skin cancer prevention by a Naval Policeman in the late 1980s who prevailed upon the then Chief of Naval Personnel to introduce the broad-brimmed hat now worn by all ranks. 7 I note incidentally from recent correspondence to The Army’, that the application of DI(G) PERS 16-10 still leaves some room for improvement. 8
Of the other 20 deaths, nine related to motor vehicle accidents, one senior officer died in a light aircraft crash, five were due to suicide and the other five to a variety of natural causes.
Suicide
The question of the relationship between service life and suicide is one that is difficult to be dogmatic about. ADF data confirms that the incidence of suicide is less than that of the general Australian community. 9 A history of prior psychiatric illness and unemployment are known risk factors for suicide; risk factors that should not be a problem for the serviceman (and they are nearly all males).
Thus, the possibility that the stresses of modern service life would constitute a contributory factor in some cases of suicide cannot be discounted.
Service related mortality 1972 – 1998
The tragedy onboard HMAS Westralia in May 1998 reminds us once again how much fire at sea is feared and respected by Naval personnel. Three sailors and one female mid shipman were killed in this blaze and a number of other personnel sustained non-life threatening burns.
Other deaths at sea since 1972 are listed at Table 1.
| Year | Unit | Incident | No |
|---|---|---|---|
| 1972 | CDT | Dive Training | 1 |
| 1975 | HMASArrow | Cyclone Tracy- Darwin Harbour | 2 |
| 1976 | CDT | Dive Training accident | 1 |
| 1981 | HMASOnslow | Toxic gas (Diesel engine run-on) | 1 |
| 1983 | CDT | Air Mix Dive | 1 |
| 1984 | HMAS Torbuk | Toxic gas (sewerage) (Naval Cadet) | 1 |
| 1985 | HMAS Stalwart | Toxic gas – 60 + casualties | 3 |
| 1987 | HMASOtama | Man overboard | 2 |
| 1992 | HMAS Success | Fall down lift well | 1 |
There have also been a number of near misses including another toxic gas incident onboard HMAS Otama (1982) and two episodes where six sailors have been swept overboard from Destroyer Escorts Torrens and Swan) during refuelling at sea (RAS) operations in rough weather. Fortunately, all were rescued although a number sustained physical and psychological trauma.
Mortality in the Fleet Air Arm
Considering the complexity of naval aviation operations, it is testimony to the skills of naval aviators (and to the engineering excellence of the Martin Baker and Douglas Escapa rejection seats) that there have been only five aircrew who have been killed in naval aircraft operations since 1970. 10
One of these was the pilot killed in the winch training accident in 1995. Two were killed in Skyhawk crashes and two aircrew men (including a RAAF medical assistant) died when their Wessex ditched in Bass Strait in 1983 whilst undertaking Oil Rig Protection operations.
Once again, there have been a number of ‘near misses’ such as the loss of a Sea King which disintegrated around the two pilots on impact with the water during a night approach to HMAS Melbourne, and the near loss of a Sea Hawk from HMAS Danuin during work-up for the Persian Gulf (Operation Damask) in 1991. This aircraft took off from the flight deck at night still attached to the RAST recovery cable. Although the system is fitted with a weak link that is designed to part at 6,000 lbs of tension, this failed and the cable parted instead at the drum. Fifty feet of cable arced through the rotor disc damaging all main rotor blades and narrowly missed the tail rotor. The crew were unaware of the damage to their aircraft until they landed back on deck.
Service accident related mortality 1972 – 1998
A total of 23 personnel have therefore died in the course of their naval duties from accidents during this 27 year period. Whilst any accidental death is one death too many, for those familiar with the environment and intensity of operations in the Fleet, one could say it reflects credit on the standards of training and levels of safety consciousness extent that there have not been more.
This data does not include personnel killed in motor vehicle accidents. Analysis of data in 1997 showed that for the 10 year period from 1986 – 95, the crude death rate from motor vehicle accidents was 24.3 per 100,000 per year compared with Australian community rates of 18.6 in 1985 reducing to 11.2 in 1995.11 The author postulated a number of reasons why this rate should be greater for the Navy including the percentage of RAN personnel in the high-risk age group, ready access to cars, and a proclivity to drive long distances on leave and on posting.
Invalidity from the RAN
The second set of statistics that have some validity are those relating to personnel being invalided or separated from the (permanent) Service on medical grounds.
In the six year period from 1991 to ’96, at total of 316 personnel were discharged on medical grounds from the RAN. A further 150 have been discharged in the 18 months to June 1998.
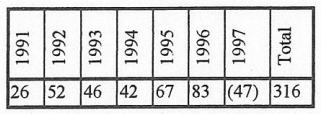
Table 2. Personnel by validated from the RAN 1991 – 1996. *Figures for 1997 are from January to June
The latest figures available are for the financial year 1997/98 when a total of 103 personnel were discharged. Given that the number of personnel in the RAN has been gradually reducing, the trend towards increasing separation via invalidity is notable.
In this most recent twelve-month period, 74 males and 29 females were invalided. This proportion of females (28%) contrasts with the 15.3% of females in the permanent Navy. 12 Personnel were predominantly from junior ranks with an average age of 26.8 years and average length of service of 6.7 years. Only one of the discharges in the female group was related to a complication of pregnancy, and none were due to a gender-specific (gynaecological) cause.
The commonest cause of invalidity was musculoskeletal conditions with lumbar spinal problems predominating. 13 The second most common cause was for psychiatric reasons.
Changing criteria for invalidity
Particularly since the Defence Reform Program has focused attention on personnel maintaining readiness for deployment, the criteria for invalidity have changed. There will necessarily be differences between the Services because of their different operating environments. A soldier is unlikely to be discharged from the Army for seasickness, although with the new emphasis on amphibious operations, that may not be true in the future.
Whilst every effort is made to avoid the unnecessary loss of highly skilled personnel, there is now less flexibility with postings to retain those who are unfit for sea. Because of the variations in the sea-shore ratio between ranks, invalidity is more likely to be the outcome of permanent disability for those who are junior sailors and officers. The discharge and invalidity process is thus a dynamic one. It is being continually refined, and emphasis is now being given to ensuring that the transition to civilian life is as smooth as possible. Early liaison with the Department of Veterans Affairs where an entitlement exists, is an important part of this process.
I think that it is fair to say that service health professionals incompletely understand the complexities of the disability, invalidity and compensation schemes.
As far as assessment of cause for the reason for the invalidity (service or non-service related), and importantly for the degree of disability (which determines the type of invalidity benefit), presiding medical officers make recommendations based upon best available guidelines, but the actual decision of course rests with the DFRDB and MSBS boards. At present, these authorities provide no feedback to the final medical board medical officers. There would be merit in providing such information in order that service medical officers are able to make informed recommendations that are in the best interest of the individual and the authorities.
Injury and serious injury in the RAN
In the same four-year period from 1994-97, a total of 1,040 ‘serious injuries’ were reported to the Occupational Health & Safety Directorate. Superficial perusal of this data indicates that the vast majority of these were due to sporting injuries, and also would not really be classified as serious. The current version of serious personal injury (SPI) includes all those incidents where a doctor is consulted. As this occurs as a matter of course in the military, it has the potential for over classification of the severity of the injury, and steps are underway to make the classification more meaningful.
Compensation premiums
One statistic that should give some indication of adverse health consequences of service life is the costs in compensation. Unfortunately there is no agreed way in determining costs due to compensable illness and injury. It is however very likely that these costs:
-
- will be substantial; and
- do not currently have the required visibility at the commander level as they are either ‘below the line’ costs or transferred to other agencies such as DVA.
The ANAO report of 1997 estimated the annual cost of ADF injury and illnesses to be somewhere between $210m and $840m. 14 This rather broad range included direct costs of $130m (pre-discharge costs $60m and post-discharge costs $70m), and indirect costs of between $80m and $710m.
Given that these figures are not included in the overall estimate of ADF health care ($400m – $600m), it is not surprising that the health services have come under close scrutiny in a number of areas following release of the report.
The Directorate of Occupational Health and Safety is able to provide some data relating to the costs of compensation. 15
The outstanding liability for Defence was estimated by the Australian Government Actuary to be $727.5m as at 30 June 1997. This figure attempts to take into account claims for injuries that have been sustained but have not yet been submitted. This does not include the costs relating to lost productivity, medical and rehabilitation cost provided in-service.
Of the three Services, on a per-capita cost, Army generates the most payments followed by Navy and then the Air Force.
Because of changing legislation and claims patterns, it is difficult to make comparisons from year to year.
It is of interest that in the case of the toxic gassing on board HMAS Stalwart in 1985, 35 of the 50-plus casualties have submitted claims for compensation for a variety of injuries, mainly psychological and in some cases, for organic brain damage. The recent submission of some of the claimants follows the successful challenge to the ComCare legislation that would have statute-barred such claims. Some settlements have been already made with pay-outs of the order of $250,000. Others are subject to confidentiality clauses.
Full steam ahead into the 21st century
The fleet of the 21st century will not only be much different from the fleet when I entered service, it will also operate in a much different environment.
Some of the problems facing our men and women at sea during peace-time training and when deployed on operations include:
-
-
- changing sea-shore ratios with increasing commitments that may conflict with family life;
- the concept of ‘minimal manning’ leading to potential problems associated with:
- watchkeeping; 16
- storing ship;
- armament handling;
- multi-skillings;
- gender and social issues; 17
- environmental threats;
- non-ionising radiation;
- asbestos.
-
Asbestos
The presence of asbestos in navy ships has been a matter of concern at least since 1968. 18 It gained widespread publicity following the premature retirement and subsequent death from mesothelioma of the Governor of NSW in 1990.
Following from recommendations in a detailed review (the Enfield report) an asbestos litigation cell was established in Sydney. This cell has documented a steady increase in claims for assessment from 1994/95 onwards; 19 Navy (by Service- including navy civilians) and NSW (by state) have consistently dominated such claims.
Until 1990/91, asbestosis was the dominant illness, however from 1992/93, mesothelioma has become the most common disease. Disbursement of fees for compensation and legal (AGS) costs peaked in 1995/96 at $5.4m. Anticipated changes to dust compensation law, which intends to end a bar on general damages, may lead to a further surge in claims.
A further outcome of the Enfield report was to draw together under the one Defence Instruction General, 20 the 24 different technical and health policies then existing in the three Services and Defence civilian areas. Navy has spent and continues to spend significant sums of money on either removing, or rendering safe by sealing, asbestos in its ships. 21 The policy is considered to be based upon the best available scientific information, and personnel can now be reassured that service on such ships does not carry any significant risk of acquiring an asbestos related illness. Nonetheless, the perception of risk is one that is not as easily removed.
RAN health doctrine
RAN health doctrine is spelt out in detail in the technical publication ABR 1991 Volumes 1 and 2. The origins of this publication stem from the Royal Navy, however, both volumes have been extensively adapted over the past 30 years to reflect Australian requirements. A reading of its contents reveals a comprehensive health delivery policy with a strong focus on preventive and occupational health strategies. This publication is progressively being taken over by tri-service technical health publications.
A high level of health care delivery (medical and dental) both shore and afloat is a persisting theme of Medical Journals and Medical Logs. The Navy’s ability to provide a sophisticated level of health support at sea will be significantly enhanced by the commissioning into service the two Level three surgical support facilities in HMAS Manoora and Kanimbla.
Summary and Conclusion
As in the case of most military forces in the world, the ADF is proceeding down the path of rationalisation, integration and force reduction draw-down at the same time it is increasing its reliance upon use of technology and of the Reserve force.
This study of data obtained from health records indicates that the Navy has been well served by its Operational Health Support and OH&S policies developed over the years as evinced by low morbidity and low mortality figures despite frequently operating in highly dangerous environments. Vigilance will be required to ensure that this good record is maintained for the future given the changing nature of service life in the maritime environment.



