
Abstract
Casualties caused by injuries have a major impact on the readiness of the Australian Defence Force (ADF). The Department of Defence has developed a system for reporting occupationally related illnesses and injuries. Data from the DEFCARE database and a wide range of other data have been analysed to determine the leading causes of injury and illness as well as the associated costs. During financial year 97/98 over 32,000 working days were lost due to injuries. In addition, over $100 million was spent on workers compensation costs. The five activities associated with the highest number of working days lost were all related to physical training and sports. Modifications to the physical training program at 1 Recruit Training Battalion were associated with dramatic reductions in the injury presentation rate and the number of male medical discharges. Further development of this type of approach should help the ADF to minimise preventable injuries in the future.
Introduction
Casualties caused by injuries have a major impact on the readiness of the Australian Defence Force (ADF). Therefore, the ADF is seeking to capture data, which will assist in determining priorities for injury prevention, designing specific interventions, and measuring progress based on implemented interventions.
Methods
The Australian Defence Force (ADF) is conducting a major study to quantify the current health status of the Force as quantitatively as possible. This project, the ADF Health Status Report, began with the compilation and analysis of a wide range of data. The desired outcomes from this process include setting health support polities; developing illness and injury prevention strategies; and beginning the process of monitoring progress toward desired health outcomes.
The Department of Defence has developed a system for reporting occupationally related accidents and incidents. The following data from workplace injuries, illnesses and incident reports are recorded in the DEFCARE database: the nature, location, agency and mechanism of injury; the activity engaged in when the injury occurred; and other information on factors which may have contributed to injuries. One of the most useful features of the DEFCARE database is the capture of working days lost (WDL) associated with each reported casualty in terms of days in hospital, days off all duties, and days of light-duty. This provides an important measure of the impact of various injuries and illnesses on personnel availability. Financial Year (FY) 97/98 was the first year for which data was compiled in the DEFCARE database.
Data on workers compensation claims in the ADF was obtained from the Military Compensation and Rehabilitation Service (MCRS) which administers workers compensation in the ADF. Although efforts are currently underway to integrate workers compensation into the DEFCARE system, this was not achieved as of FY97/98. However, some data was available on the condition for which compensation was claimed in terms of the part of the body affected.
Because ADF personnel must maintain a high standard of fitness, each Service has the light to retire members on the grounds of invalidity, that is, a physical or mental incapacity to due their duties. There are three classifications of invalidity retirements: Class A (60% or greater incapacity), Class B (30% to 59% in capacity), and Class C (less than 30% incapacity). Data on invalidity retirements was obtained from the Defence Force Retirement and Death Benefits (DFRDB) Scheme and the Military Superannuation and Benefits Scheme (MSBS). Both the DFRDB and MSBS maintain statistics on the cause of invalidity in terms of the body system affected.
Each of the Services in the ADF collects data on hospital admissions, including the reason for admission using International Classification of Diseases Edition 9 (ICD-9) coding. This allows for a determination of the number of admissions associated with injuries and musculoskeletal diseases and disorders. Each of the military Services also maintains records of deaths due to all causes. Based on this data it is possible to ascertain the number of deaths resulting from accidents and injuries.
In addition to the aforementioned sources of data, the ADF Health Status report included a review of previously collected data and studies on injuries in the ADF. Significant in this regard was a major report on injuries in the Australian Army from 1987-1991 by Rudzki. 1All the sources of data mentioned above were analysed in an attempt to develop a comprehensive picture of patterns of injuries and illnesses in the ADF. Where possible, an attempt was also made to establish causal relationships in order to guide casualty prevention strategies.
Results
In FY97/98 there were 5038 casualties among full-time military personnel reported to the DEFCARE database, which represents a rate of 91 per 1000 per year (9.1% of the Force). The resulting WDL was 32,644 (148 work years), including 1216 days in hospital, 6287 sick days, and 25, 141 light-duty days. In FY97/98 1067 casualties among part-time military personnel were reported to DEFCARE resulting in an additional 2680 WDL. When calculated in terms of full-time equivalents the casualty rate among part-time forces was 28.5%.
The activity groups associated with workplace injuries and illnesses among full-time personnel are presented in Figure 1. Work related activities accounted for almost one-third of all casualties reported. Sports activities were also associated with approximately one-third of casualties. Physical training was the third leading activity group in terms of the number of casualties produced. Military training and motor vehicle accidents played a smaller, but still important role.
The individual activities associated with the highest number of casualties included the following: physical training (18.2%), walking (non-sport and fitness) [6.7%], rugby union /league (5.0%), equipment maintenance (4.6%), touch football (4.1%), soccer (3.9%), stores handling (3.9%), driving (3.8%), fighting (3.4%), ship maintenance (2.8%), running/jogging (2.6%), cleaning (2.5%), Australian Rules football (2.4%), and basketball/netball (2.3%).
However, in terms of priority for prevention the individual activities associated with the highest WDL are of greatest concern. Figure 2 presents a summary of activities associated with the highest percentage of WDL. The five leading activities associated with WDL are physical training (PT) and four sports activities, including touch football, soccer, rugby union/league, and running/jogging. Several other sports activities were associated with the highest proportion of WDL. Military training activities, such as marching and parachuting, were also important contributors to WDL. Walking and stores handling were work related activities associated with relatively high WDL.
Sprains and strains of joints and adjacent muscles was by far the leading injury nature associated with lost working days and accounted for almost 30% of all casualties and 31% of WDL. Disorders of muscle, tendons and other soft tissues and fractures were also major contributors to WDL with each accounting for approximately 18% of days lost. Dislocations and dorsopathies each accounted for approximately 5% of WDL. The types of injury associated with the highest WDL are not surprising given the activities associated with the highest WDL.
Figure 3 presents a summary of the location of injuries and illnesses in full-time military personnel reported to DEFCARE in FY97/98. Again it is not surprising that lower limbs were affected in one-third of casualties given the types of activities associated with the highest rates of casualties. Lower limb injuries are associated with over 50% of WDL. Upper limbs were affected in 22% of casualties reported and accounted for 20% of WDL. The third highest body location to be impacted was the trunk, which accounted for over 15% of casualties and WDL. All other body locations were much less likely to be affected.
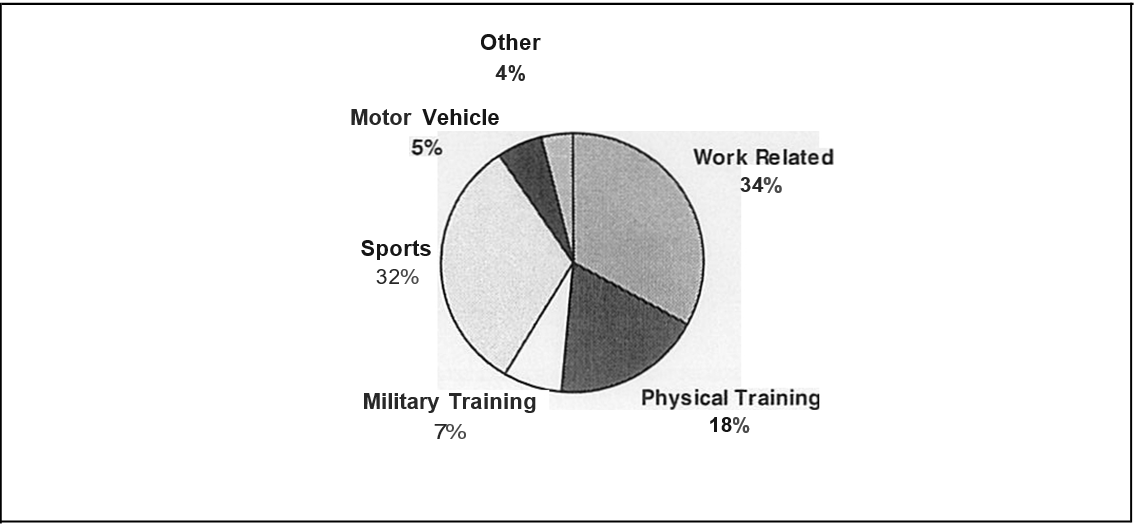
Figure 1. Workplace Related Casualties by Activity Grouping
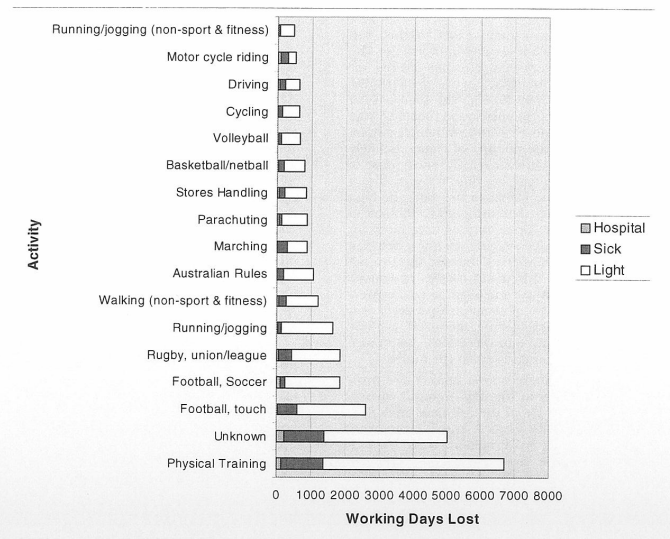
Figure 2. Individual Activities Associated with the Highest Number of Working Days Lost
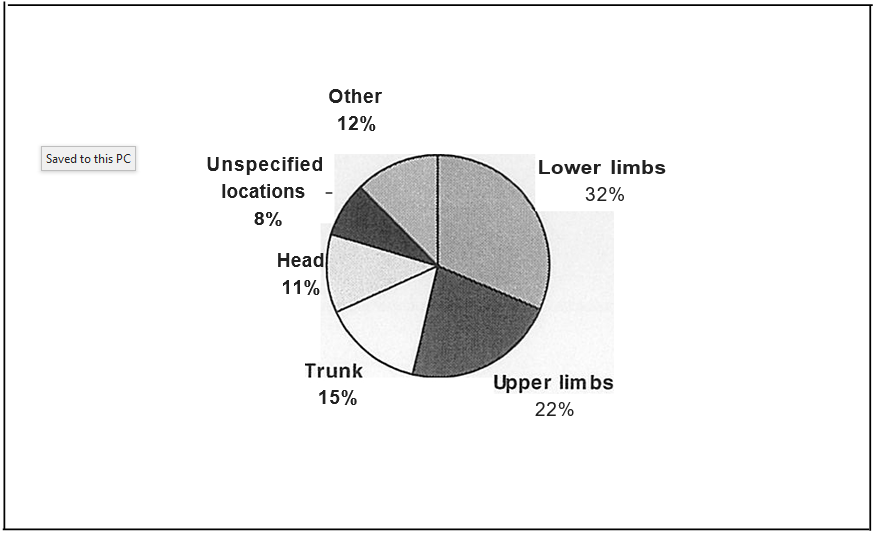
Figure 3. Injury Location Group Summary for ADF Workplace Injuries and Illnesses
Workers compensation costs in the ADF have seen significant escalation overtime. The number of workers compensation claims received almost doubled between FY90/91 (3208) and FY97/98 (6285). The total cost of military worker’s compensation benefits was $101.23 million in FY97/98. Although part of the increase in the number of claims is likely associated with greater client awareness of benefits and the long lag time between injury and submission of claims in the ADF, the high cost of work-related injuries and illnesses in the ADF is clear. Knee injuries accounted for 19.4% of compensation claims between FY92/93 and FY96/97. Other leg injuries accounted for an additional 18.7% of claims. Back and arm injuries accounted for an average of 15 and 13% of claims, respectively over the five-year period. Integration of workers compensation data into DEFCARE should provide for useful comparisons in the future.
In FY97/98 there were a total of 574 invalidity retirements in the ADF from all causes. This represents 1% of the full-time force. The annual liability for Class A and B retirements in FY97/98 was $67.6 million. While Class A retirements have held relatively steady over the past five years, Class B retirements have steadily increased over the past four years. Class C retirements, which are by far the most numerous, fluctuated considerably with a range of 158 to 264 per year. Diseases and disorders of the musculoskeletal system accounted for 62% of Class A and B retirements and 63% of Class C retirements in FY97/98 under MSBS. A total of 37% of all invalidity retirements were associated with diseases and disorders of joints and 16.5% were associated with spinal injuries.
Based on a review of hospital admission data over the last several years, the average number of admissions related to injuries and poisonings or musculoskeletal diseases and disorders was over 2000 per year. Australia’s Health 19982 indicated that the average cost per admission for musculoskeletal diseases and disorders and injuries, poisonings, and toxic effect of drugs was $3369 and $2307, respectively. Thus, the cost of hospitalisation of ADF personnel for such injuries and illnesses is estimated to be millions of dollars. The Australian National Audit Office (ANAO) has estimated that the total cost of injuries in the ADF is between $210 and $840 million.3 Furthermore, on average, 22 ADF personnel die as a result of accidents and injuries every year with motor vehicle accidents taking the greatest toll on life.
Given the major costs associated with workplace injuries and illnesses in the ADF, the need for focused injury prevention efforts are clear. Based on a thorough analysis of available information it became clear that substantial numbers of injuries and illnesses (particularly musculoskeletal diseases and disorders) are preventable. PT and sports injuries should receive the highest priority for prevention efforts. Military training activities such as marching and parachuting should also receive attention along with work-related activities associated with high numbers of casualties (eg. walking, maintenance, and stores handling).
The rest of this paper will focus on the ADF’s initial efforts in seeking to address the problems of PT and sports injuries.
Table 4 provides a profile of the nature, location, and mechanism of injury for each of the leading causes of WDL and indicates the proportion of casualties associated with each.
Table 4. Profile of the Activities Associated with the Highest WDL
| Activity | Nature of Injury | Bodily Location | Injury Mechanism |
|---|---|---|---|
| Physical Training | Sprains & strains (49%) Disorders of muscles, tendons and soft tissues (12%) Fractures (1 0%) |
Lower limbs (48%) Upper limbs (20%) Trunk (18%) |
Body stressing (34%) Falls, trips & slips (29%) Hit by moving objects (15%) |
| Touch Football | Sprains & strains (44%) Disorders of muscles, tendons and soft tissues (17%) Fractures (II %) |
Lower limbs (56%) Upper limbs (26%) Trunk (10%) |
Falls, slips & trips (34%) Body stressing (22%) Hit by moving objects (15%) Hitting objects (14%) |
| Rugby Union/League | Sprains & strains (35%) Fractures (16%) Disorders of muscles, tendons and soft tissues (14%) Dislocation (8%) |
Upper limbs (31%) Lower limbs (31%) Head (14%) Trunk (14%) Neck (7%) |
Hit by moving objects (66%) Falls, slips & trips (II %) Hitting objects (10%) Body stressing (8%) |
| Soccer | Sprains & strains (48%) Fractures (20%) Disorders of muscles, tendons & soft tissues (11%) |
Lower limbs (69%) Upper limbs (13%) Trunk (7%) |
Hit by moving objects (47%) Falls, slips & trips (19%) Hitting objects (15%) |
| Running/jogging | Sprains & strains (52%) Disorders of muscle, tendons and soft tissues (17%) Fractures (8%) |
Lower limbs (78%) Upper limbs (7%) Trunk (7%) |
Falls slips & trips (40%) Body stressing (32%) |
Citing a report on sports injuries in Australia by the Centre for Health Promotion and Research, Rudzki noted that based on questionnaires completed by coaches, administrators and medical staff, a mean estimate of 30-50% of sports injuries were regarded as realistically preventable.1 Rudzki also cited an Australian Sports Medicine Federation study indicating the major causes of sports injury are human error (54%), terrain (31%), and equipment (15%).1 Rudzki concluded that the main areas of manipulation are education and modifying the environment with coaches and trainers being the people deemed most important in preventing sports injuries. The ADF must learn from training and conditioning programs of professional and top amateur sports programs how to minimise preventable injuries. In essence, the ADF must learn to train smarter to minimise risk. This will require greater
education of commanders and all personnel regarding the benefits, risks and prevention strategies for minimising injury.
| Risk Factor | Level of Evidence |
|---|---|
| Age over 24 years | Grade B level lib |
| Low or average physical activity prior to training | Grade B level lib |
| Female gender | Grade B level III |
| Smoking>10 /day | Grade B level lib |
| Hyperpronation of foot | Grade C level IV |
| Total amount of marching/running (military training) | Grade B level lib |
| Running frequency> 3 days/week for 30 mins | Grade B level lia |
| Running duration >30 mins for 3 days per week | Grade B level lia |
Where primary prevention efforts fail, the ADF must have the means to aggressively manage injuries to ensure they are completely healed and do not become chronic problems that can eventually lead to medical discharge. Physiotherapy is extremely important as a means of secondary prevention. However, when other means fail, the ADF must have strong rehabilitation programs in place.
A case study at 1 Recruit Training Battalion (1 RTB) by Rudzki and Cunningham provides an idea of the potential impacts that smarter training can have. 5 Medical staff at l RTB was able to convince commanders at the Army establishment for initial recruit training that changes in physical training could result in fewer injuries while still providing rigorous training and physically fit recruits. Changes in the PT program included the following: cessation of road runs, introduction of 400-800m interval training, reduction in test run distance from 5km to 2.4km, standardisation of road marches, and introduction of deep water training. These changes address several of the risk factors in Table 5. The results of the uncontrolled observational study included a 46.6% reduction in the total injury presentation rate for medical treatment. In addition, the annual rate of medical discharges among males decreased by 40.8% resulting in an estimated savings of over $1.2 million.
Conclusions
Injuries and illnesses have a major impact on the ADF both in terms of decreased personnel availability and monetary costs. Physical training and sports injuries should receive the highest priority for prevention efforts. Based on a survey of relevant literature and the case study at 1 Recruit Training Battalion, it appears that substantial numbers of injuries and illnesses can be prevented through smarter training. Resources invested in prevention efforts are likely to be extremely cost-effective as well as increasing Defence readiness.