
R Lain, M Page
Abstract
Background: Dental records of HMAS Sydney II ( lost in 1941) were examined during previous research on the Unknown Sailor’s possible identity. The poor state of oral health was noted. Comparison with a modern-day cohort of crew from Sydney IV was considered a potentially useful analysis noting military population dental data from the late 1930s is relatively rare.
Purpose: To quantify the difference in oral health between RAN members in the 1930s and the early 2000s.
Materials and Methods: 256 records on entry to the RAN from Sydney II were compared to 114 records from Sydney IV. Age on entry was recorded. Parameters used were the DMFT score (number of Decayed, Missing or Filled Teeth) and T-health score (a composite score based on DMFT score indicating quality of dental function).
Results: Mean age on entry was 19.5 years (median 18 years) for Sydney II and 21.5 years (median 19 years) for Sydney IV. For Sydney II, 20 of 256 (7.8%) members had a DMFT score of 0 (no Decayed, Missing or Filled Teeth); for Sydney IV 22 of 114 (19%) had a DMFT score of 0. For Sydney II, 10% of the crew had a DMFT of 16 or more; in Sydney IV only one member had a DMFT of 16 or more. The mean T-health score for Sydney II was 25.5; and 27.8 for Sydney IV.
Conclusion: Historical data has significant limitations for analysis. However, DMFT and T-health scores give a broad indication of oral health. This study supports and quantifies the anticipated improvement in oral health in the RAN from the late 1930s to today.
Introduction
On 19 November 1941, HMAS Sydney II, a modified Leander class light cruiser of 6700 tons, was lost following a battle with the disguised German raider HSK Kormoran off Carnarvon, Western Australia. There were no survivors among the 645 crew. Three months later a Carley float was detected off Christmas Island and retrieved. The float contained a decomposing body. The remains were buried on Christmas Island; however, partly due to the island’s occupation a few weeks later by the Japanese, the location of the grave was lost. A RAN-led team located the grave in 2006 and recovered the remains of what had become known as the Unknown Sailor. Since then, there has been ongoing activity to identify the remains, utilising the three stand- alone identification modes recognised by Interpol: odontology, fingerprint techniques and biology (DNA techniques). These are informed and supported— particularly in this case of historical remains—by physical anthropology techniques and property analysis (uniform, equipment, grave contents). At the time of publication of this article, the Unknown Sailor—the only remains ever recovered from HMAS Sydney II—remains unidentified.
While the original 645 dental records of those members of HMAS Sydney went down with the ship in 1941, 256 members of Sydney’s crew had surviving supplemental dental records, collected at their time of entry to the RAN. These were archived at the Sea Power Centre in Canberra. Facsimiles of these records were made available for a second pass analysis in the hopes of leading to the potential identification of the Unknown Sailor. During this process, it was noted that the records reflected a relatively poor standard of oral health. RAN members’ oral health in the early 1900s, while long assumed to be poorer than that of the modern population, has never been formally compared to oral health in the current RAN. It was thought that it may be useful to analyse these records, which represent some of the earliest military dental data available, in order to support some of the assumptions made about dental health in the 1930s. The records from Sydney II were compared with those of the recently decommissioned HMAS Sydney IV, an Adelaide class guided missile frigate of 4100 tons, to gain a quantitative and qualitative assessment of the observed difference in oral health status of serving members in the mid- 1930s to those of present day.
Materials and methods
Facsimiles of the 256 available on-entry dental records from HMAS Sydney II were collated. The number of decayed, missing and filled teeth (DMFT score) was noted for each record, in addition to age at the time of entry. T-health scores were also calculated as a measure of comparative health and dental function (see Discussion for explanation of DMFT and T-health score).
Ethical approval for a review of the HMAS Sydney IV records was obtained from the Australian Defence Health Research Ethics Committee. The dental health at the time of entry for each member was recorded for this population using the DMFT index. Features such as the presence of dentures were also noted. Fissure sealants, a modern preventative treatment modality that seals deeply fissured occlusal (biting) surfaces of teeth that are susceptible to decay through the application of a restoration, commonly a composite resin (often without the need to remove any tooth structure) were not recorded as restorations for this study. Data from the two populations were then analysed to obtain quantitative measures of oral health for both populations to allow valid comparison.
Results
Population data obtained from the 256 HMAS Sydney II on-entry records are summarised in Table 1. Mean joining age was 19.5 years (median 18 years). The overwhelming majority of members were rated sailors, with only two surviving officer records. Only 20 out of 256 members (7.8%) with dental records had no decayed, missing or filled teeth charted (DMFT = 0). Just over a third (36%) had a DMFT of less than four, and approximately 10% had a DMFT of 16 or more. Three of the members were completely edentulous (DMFT = 32), with the least partially dentate member having only four teeth remaining. Very few of the partially dentate members had a denture recorded in the dental record on enlistment. Thirty-two members wore a denture. Of the 256 members, 243 had no restorative work (fillings) charted on entry,
Table 1 – Summary Data
HMAS Sydney II (n=114)
| SCORE | DMFT | D | M | F |
|---|---|---|---|---|
| < 4 | 92 | 212 | 126 | 247 |
| 4 to 7 | 69 | 33 | 75 | 4 |
| 8 to 11 | 48 | 6 | 25 | 2 |
| 12 to 15 | 23 | – | 10 | – |
| 16 to 19 | 13 | 1 | 8 | – |
| 20 to 23 | 3 | – | 3 | – |
| 24 to 27 | 2 | – | 1 | – |
| 28 + | 4 | – | 4 | – |
HMAS Sydney IV (n=256)
| SCORE | DMFT | D | M | F |
|---|---|---|---|---|
| < 4 | 52 | 101 | 97 | 84 |
| 4 to 7 | 39 | 10 | 13 | 23 |
| 8 to 11 | 16 | 3 | 4 | 5 |
| 12 to 15 | 4 | – | – | 1 |
| 16 to 19 | 3 | – | – | 1 |
| 20 to 23 | – | – | – | – |
| 24 to 27 | – | – | – | – |
| 28 + | – | – | – | – |
HMAS Sydney II
| SCORE | DMFT | D | M | F |
|---|---|---|---|---|
| < 4 | 36% | 84% | 50% | 98% |
| 4 to 7 | 27% | 13% | 30% | 2% |
| 8 to 11 | 19% | 2% | 10% | 1% |
| 12 to 15 | 9% | – | 4% | – |
| 16 to 19 | 5% | – | 3% | – |
| 20 to 23 | 1% | – | 1% | – |
| 24 to 27 | 1% | – | 1% | – |
| 28 + | 2% | – | 2% | – |
HMAS Sydney IV
| SCORE | DMFT | D | M | F |
|---|---|---|---|---|
| < 4 | 46% | 89% | 85% | 74% |
| 4 to 7 | 34% | 9% | 11% | 20% |
| 8 to 11 | 14% | 3% | 4% | 4% |
| 12 to 15 | 4% | – | – | 1% |
| 16 to 19 | 3% | – | – | 1% |
| 20 to 23 | – | – | – | – |
| 24 to 27 | – | – | – | – |
| 28 + | – | – | – | – |
HMAS Sydney II
| DMFT | D | M | F | |
|---|---|---|---|---|
| Mean | 6.7 | 1.5 | 5.1 | 0.1 |
| Mode | 3.0 | 0.0 | 2.0 | 0.0 |
| Median | 5.0 | 1.0 | 3.0 | 0.0 |
HMAS Sydney IV
| DMFT | D | M | F | |
|---|---|---|---|---|
| Mean | 4.8 | 1.2 | 1.1 | 2.4 |
| Mode | 0.0 | 0.0 | 0.0 | 0.0 |
| Median | 4.0 | 0.0 | 0.0 | 1.5 |
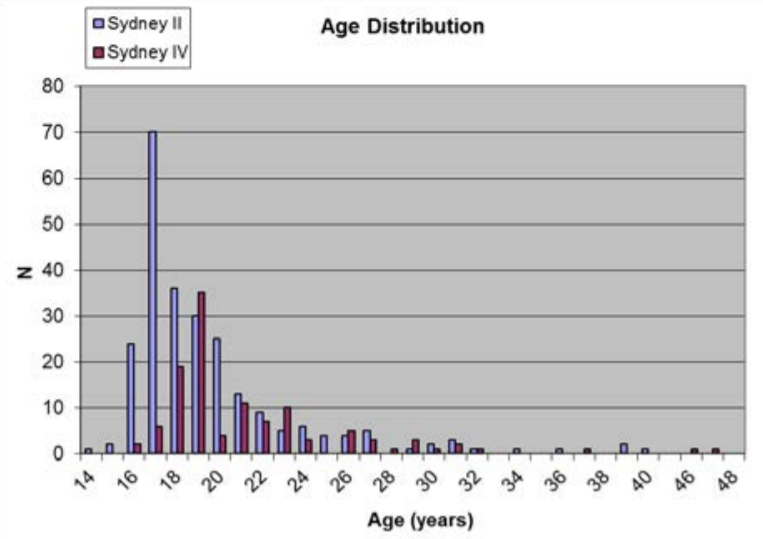
Figure 1 – Age distribution of samples
with decayed and missing teeth accounting for the majority of the DMFT scores. Two hundred and eighteen members had one or more missing teeth on entry, and 134 had one or more decayed teeth.
One hundred and fourteen documents were obtained from HMAS Sydney IV, representing 100% of posted strength at the time of the study. Population data are likewise summarised in Table 1. The age distribution was similar to that of Sydney II, with a skew towards younger members (Figure 1). Mean age at enlistment was 21.5 years (median 19 years). From a total of 114 members, 22 had a DMFT score of 0 on entry (19%). The maximum DMFT was 18, represented by 18 filled teeth in a member born in the 1960s who joined as a 19-year-old. The highest number of missing teeth in any one member was nine. Fifty-six members had one or more decayed teeth, 78 members had one or more filled teeth, and 46 members had one or more missing teeth.
While the mean DMFT scores on entry differed between Sydney II and IV populations by a relatively small degree (6.7 vs 4.8, p < 0.001), the relative progression of DMFT scores differed markedly between the two populations according to age, as can be seen in Figure 2. The mean DMFT for those in the 26+ age group was 14.1 for the Sydney II population (n=21) and 5.8 for the Sydney IV population (n=19). T-health scores unsurprisingly indicate that the Sydney II population had overall poorer dental health as a cohort compared to the modern population in Sydney IV. The mean T-health score in the Sydney II population was 25.5, compared to 27.8 for the Sydney IV group.
Discussion
The data presented here confirm other studies on historical military populations. The overall dental health of recruits was significantly poorer during the mid-20th century compared to that of today.1,2,3 For members in the early to mid-1900s, the vast majority of early dental treatment did not involve restorative treatment. Data collected from the entry examinations of 350 17-year-olds between 1928 and 1933 showed that 88% of the first molars were affected by caries, 68% being already extracted or
Figure 2 – Age-distributed DMFT Scores

classified as ‘irreparable’ requiring extraction. A further study by the same author of 1750 18-year- olds on entry between 1937 and 1938 found 52% of first molars classified as ‘irreparable’.4 Only 10 members (<4%) of the HMAS Sydney II crew had received a restoration by the time they entered service. This can be compared to Sydney IV’s crew, where 78 (70%) of members on entry had received a restoration of some sort. This is reflective of the shift in community attitude towards dental health in the last 80 years, in combination with the advent of government-sponsored public dental programs such as school dental services, programs targeted at oral health in children and later fluoridation of the water supply in most of Australia, beginning in Tasmania in 1953 and other states in the 1960s and 70s. The author of the 1936–1938 study noted the drop in the percentage of teeth classified as ‘irreparable’, and considered that this was due to the increased activities of school dentists and the improved means of transport of dental equipment.4
The DMFT index is a broad indicator of oral health. A score representing no dental disease, no restorations (fillings) and no missing teeth is indicated by DMFT = 0. A member with a full complement of 32 teeth and four restored teeth would have a DMFT = 4. A member with healthy teeth and no restorations but with all the third molars (wisdom teeth) removed would also have a DMFT score = 4. The worst possible score, indicating either decay or restoration in every tooth, or every tooth missing, or some other combination of these events, would be a DMFT score = 32. While this composite number does not allow this distinction to be drawn, the DMFT index can be split into its parts (i.e. D=2, M= 2, F= 1, DMFT= 5), in order to refine this detail better. While the DMFT index provides only a broad assessment of dental health, it was selected in part because of the limited data contained in the dental records of the crew of HMAS Sydney II.
A study of Royal Australian Air Force personnel1 found that 57% of the mean DMFT score of 19.5 was attributable to missing teeth during 1939–1945. The present study suggests that the mean DMFT score on entry was far lower in the RAN in the 1930s (see below). However, more of it was accounted for by
missing teeth (78%). Those with a higher DMFT score were more likely to have the majority proportion of the score accounted for by missing teeth in the Sydney II population. In contrast, in the modern sample, the majority with a DMFT score greater than 4 was accounted for by decayed and restored teeth. A study of RAN recruits in 19882 found mean DMFT scores of 4.33, 6.85 and 8.87 for members aged 15–19, 20–24 and 25–29 respectively. By comparison, the 1930s cohort represented by Sydney II demonstrates mean DMFT scores of 5.3, 7.3 and 13.0 for the same age ranges. The vast majority of missing teeth in the Sydney IV population were third molars and first or second premolars, likely extracted for orthodontic reasons rather than due to decay. In contrast, the most commonly extracted (or tooth charted as missing) in the Sydney II population was the first molar. This is not unexpected, as it is usually one of the first adult teeth to erupt around age six.
In contrast to the DMFT index, the T-health index5,6 is a composite indicator of oral health, based on the DMFT score, that provides an overall indicator of dental function. It weights missing teeth higher than decayed teeth, which are similarly weighted higher than filled teeth in order to reflect the progressive loss of function from restored through to missing teeth. The index is a reasonable indicator of dental function when compared to self-rated scales, providing that the weight of a decayed tooth is approximately twice that of a filled tooth with an assigned weight of less than 0.2. In this study, these recommendations were followed by assigning weights of 1.0, 0.2, 0.1 and 0 for sound, filled, decayed and missing teeth respectively. The highest T-health score possible is 32, suggestive of full function with a completely present and unrestored dentition. The mean T-health score in the Sydney II population was 25.5, compared to 27.8 for the Sydney IV group. It was surprising that there was a relatively small difference between the two cohorts’ mean T-health scores in this study. However, when considering the age-distributed pattern of caries, and the population’s age distribution, this appears logical, as most oral health function is lost in post- 26-year-olds (see Figure 2). For members who were 26 years of age or older on enlistment, the relative T-health scores were 17.9 for Sydney II and 26.8 for Sydney IV.
Historical data of this nature has significant limitations and is beset with issues that make drawing definitive conclusions difficult. The majority of the dental records on entry appear to have been signed off by a Medical Officer. Many forms have the notation next to the dental chart ‘Signature of Naval Dental Officer (if available)’, and this is blank or crossed through. Historically, the dental examination on entry during World War II was often conducted with a penlight or torch as part of the medical examination, rather than in a proper dental facility. It is difficult to say how accurate a Medical Officer’s charting may be under these conditions compared to that of a Dental Officer. Missing teeth and restorations (largely consisting of gold or amalgam at the time) are generally evident to those not trained in dentistry. However, the extent of decay is probably underestimated in this analysis as its detection is often difficult in the early stages, and one could assume that only obvious decay was likely to be recognised by the examining officer.
Additionally, no radiographic data were available for the Sydney II cohort. Contemporary dental examinations always consist of radiographic examination in addition to clinical examination by a Dental Officer, with radiographs able to confirm the presence or absence of teeth, particularly unerupted and hence unseen third molars in younger patients. It is unknown whether the recruits routinely had dental radiographs taken on entry—the record suggests that this was highly unlikely. It is more likely that decay has been underdiagnosed in the Sydney II population, as interproximal decay (between the teeth) is difficult to detect, particularly by non-dental clinicians, until the later stages. Individual factors such as diet and oral hygiene likely explain the rapid increase in decay prevalence seen in the over-26 population.
It is difficult to draw firm conclusions from cross-sectional caries data, as dental caries is a multifactorial disease whose epidemiology is affected by individual factors such as diet, fluoride exposure and personal oral hygiene practices. During dental development, geographic location also affects the former two of these, particularly fluoride exposure and acts as a secondary mediator that is impossible to account for in this study. Nevertheless, the use of DMFT score as a broad indicator allows a valid comparison between the crews’ dental health of HMAS Sydney II and HMAS Sydney IV, representative of military populations in the RAN in the mid to late 1930s and today.
Corresponding Author: Lieutenant Commander Russell Lain OAM RAN Russell.Lain@sydney.edu.au
Authors: R Lain1,2, M Page3
Author Affiliations:
- Sydney Dental Hospital, Oral Surgery and Diagnostic Imaging Department
- NSW Department of Forensic Medicine, Identification
- Royal Australian Navy