
C Heard, M Willcox, M Falvo, M Blatt, D Helmer
Abstract
Purpose: Performing well in combat requires military service members to be in peak physical shape. Although each branch of the United States military has fitness guidelines and assessments, there are no exact prescriptions for physical training programs. The absence of a standardised approach may lead to suboptimal physical performance and increased risk of musculoskeletal injury. To address this gap, we evaluated the feasibility of a pilot combat conditioning program based on linear periodisation.
Methods: Twenty-nine garrisoned US Marine Corps service members (25 men, 4 women; 23.5±4.4 years) enrolled in our 11-week conditioning program that was supervised by a strength and conditioning professional. Military- specific (physical/combat fitness tests) and general (treadmill-based maximal exercise test) assessments were performed at baseline and 11 weeks. Training and injury logs were maintained throughout the duration of the program.
Results: Approximately 80% (23/29) of service members completed the entire program. Cardiorespiratory fitness (Peak VO2; +8.10±10.9%; p=0.011), upper-body strength (pull-ups; +47.0±58.2%; p<0.001) and core strength (abdominal crunches; +9.2±23.3%; p=0.029) significantly increased from pre- to post-training. No statistically significant improvement or worsening was noted in any other performance assessment measure. Eight (28%) participants reported minor musculoskeletal concerns, of which only one required medical attention (injury rate 1.3 injuries/100 person-months).
Conclusion: A protocolised linear periodisation training program was feasible and demonstrated improvements in fitness in a group of garrisoned Marines with low injury rates. Other military units may benefit from a similar approach
Introduction
Military service members in combat environments are subject to physically and mentally challenging conditions making it essential that they achieve and maintain a high level of fitness. Army Field Manual (FM) 7-22 describes the physical demands that soldiers face and states that ‘all these activities of warfare and many others require superb physical conditioning’ 1 To ensure service members stay fit, each branch of the United States (US) military service has established fitness standards and fitness tests.2–4 However, these documents lack the detail needed to create a systematic training program that would increase fitness and minimise musculoskeletal injuries. For example, the Marine Corps Physical Fitness Program provides an overview for use but does not provide enough details for unit leaders to create a systematic training program.3 In the absence of clear guidelines, unit leaders may implement suboptimal programs that fail to improve fitness in service members and may even increase the risk of musculoskeletal injuries. Effective conditioning requires a balance between intense training sessions and periods of rest/recovery. Too much overload and/or not enough recovery can result in both physiological and psychological symptoms that limit performance and may cause individuals to cease participation in a previously enjoyable activity. In many non-competitive exercisers, inadequate rest/ recovery because of busy work lives, family, work and health stressors, meal skipping and poor sleep can result in overtraining syndrome.5
The prominence of musculoskeletal injuries (MSIs) among military personnel has significant repercussions on the readiness of the armed services and can result in high cost. For example, studies have shown that during Army deployments, more medical air evacuations result from non-battle activities, such as physical training and recreational sports, than from combat.6,7 The leading cause of healthcare visits for all military personnel in 2012 was MSIs, resulting in the largest number of lost duty days annually – greater than illness or any other reason.7 These injuries are often avoidable and can compromise mission success. For these reasons, prevention of MSIs is of the utmost importance for the US military.
Systematic training programs may reduce the risk of injury from physical training activities, particularly overuse injuries.8 In particular, linear periodised training programs have been used by athletes for training.9,10,11 Linear periodised programs increase load and repetitions systematically over an extended period. Usually, every fourth week is an unloading week where repetitions and load are decreased. This allows coaches to control the amount of stress put on the body. Such programs have been shown to increase physical fitness while keeping injuries to a minimum.5
To address the current gaps in fitness training among military personnel, we report the results of a pilot trial of an 11-week linear periodised training program. We explored the feasibility, safety and effectiveness of a systematic approach to physical fitness training in an active duty administrative unit of the US Marine Corps (USMC).
Methods
Population/subjects
A single garrisoned administrative unit of the USMC was targeted for this study with explicit approval from the commanding officer. All unit members were informed of the purpose and expectations of the study through written and verbal communication and asked to approach the on-site program leader to volunteer. The study was reviewed and approved by all relevant research oversight committees.
Study inclusion criteria included male and female Marines, ages 18–55 years, stationed at a USMC facility in the western US who were granted permission to participate by their chain of command. Exclusion criteria included individuals with contraindications for exercise studies according to the American College of Sports Medicine (ACSM) pre- participation screening algorithms.12 This included individuals with significant cardiovascular disease, neurological impairment/disorder, pregnancy, uncontrolled hypertension (SBP > 160; DBP > 100) or musculoskeletal injury impeding the required physical activities of the interventions. A total of 29 garrisoned US Marines were recruited and consented to participate in an 11-week combat conditioning assessment program (CCAP) from September to December 2012.
Physical conditioning program
The CCAP is a linear periodisation program starting with low-intensity and low-volume training that builds weekly. Increasing the number of repetitions, mileage and/or time spent working out alters the intensity and volume of the program. Additionally, the intensity is also increased by increasing load carriage, or the weight of the clothing or gear worn throughout the training session, such as combat boots and flak jackets. The 11-week training program evaluated in this study included one-hour sessions every Monday, Wednesday and Friday (total of 32 sessions). Intensity would build over a three-week period, while every fourth week was an unloading week, during which the intensity and the volume were decreased, allowing for active recovery. The 11-week duration balanced practical considerations with the completion of three 3-week intensity building periods with post-intervention assessment in the unloading week of the final cycle. This duration was estimated to be adequate to demonstrate changes in physical performance measures.
The 29 Marine participants were randomised into two test groups using a random number generator: high-intensity CCAP (CCAP-High) and moderate- intensity CCAP (CCAP-Mod). The two test groups differed only by relative volume of activity and total repetitions. Each one-hour session included variations of exercises derived from the Combat Conditioning Manual from the Marine Corps Martial Arts Center for Excellence, including 440-yard sprint, pull-ups, push-ups, squats, front and side planks, squat presses, lunges, woodchoppers, side toss, crunches, burpees, thrusters, bent-over row, bench press, overhead press, Russian twists, tire flips, rope climbs and more. The routines for both CCAP-High and CCAP-Mod groups are seen in Appendix 1.
Assessment
Each participant completed baseline medical screening, self-report health/behaviour instruments and physical function assessments. Medical screening consisted of height, weight, waist circumference and skinfold measurement to compute body fat percentage via Jackson/Pollock 3-site method.13,14
The physical fitness test (PFT) and combat fitness test (CFT) are the standard fitness measures used by the USMC and performance can be summarised using a total score for each (PFT range 120-300; CFT range 120-300).15 In 2012, the Marine Corps PFT included a three-mile run, a sit-up requirement (two minutes) and a pull-up (untimed) or flexed arm hang (female) requirement. The Marine Corps also utilised an annual combat fitness test to standardise the assessment of common battlefield manoeuvres. The test components included: Movement to Contact (MTC; 880-yard run in boots and camouflage uniform bottoms); Ammunition Lift (AL; maximally repeated overhead lifts of a 30-pound ammo can for two minutes); and Manoeuvre under Fire (MANUF; 300-yard standardised combat obstacle course). These standard USMC assessments were replicated as part of the study assessments, administered on separate days at baseline and conclusion of the study intervention.
Cardiorespiratory fitness was assessed using a maximal treadmill test (Bruce protocol) and performed on a separate day from PFT/CFT. A clinical exercise physiologist conducted exercise testing, supervised by a registered nurse and an independent active duty ombudsman. Metabolic and ventilatory measures were obtained breath-by- breath using a portable commercial system (Cosmed K4b2), and heart rate was measured continuously using an integrated chest strap heart monitor (Polar). Blood pressure was manually taken every two minutes. Primary variables of interest from exercise testing included peak oxygen consumption (VO2) and ventilatory anaerobic threshold (VAT), as determined using the modified v-slope method.16 Maximal effort was determined according to ACSM criteria, which included meeting two of the following: 1) respiratory exchange ratio ≥ 1.1; 2) achievement of 85% of age-predicted maximum heart rate; 3) a rating of perceived exertion of 17 or higher; and 4) no change in VO2 of 200 mL with an increase in workload. ACSM criteria were also used for test termination to ensure participant safety 17
Monitoring of participation and injuries
An on-site program leader certified as a strength and conditioning specialist and personal trainer monitored adherence to the CCAP training program and injury rate, as well as training fidelity assessment surveys and injury logs, administered to each participant after each training session. Musculoskeletal concerns were recorded at each training session on a log by the participant and confirmed by the program leader. The documentation included the specific location, context and severity of any musculoskeletal concern, whether that person sought medical attention, and if it resulted in light or no duty assignment following the injury. When participants missed sessions, the on-site program leader contacted the participant and recorded the self-reported reason for the absence. Participants were allowed to make up a missed session (either anticipated or actual) +/- one day of the scheduled session.
Data analysis
Originally designed as a randomised controlled trial comparing moderate and high-intensity training regimens, once in the field, it was clear that the small sample sizes recruited required a change in scope. Data collection plans remained unchanged, but the expectations shifted to focus on feasibility, safety and generation of pilot performance and fitness data.
The primary outcome measures for this study reflected physical performance as measured by peak voluntary oxygen consumption (VO2 peak) and PFT scores. Secondary outcome measures include CFT scores, lower body power and injury rates. Paired sample t-testing was used to detect statistically significant changes in primary outcome measures from baseline to the end of the 11-week period in the merged CCP-High and CCP-Mod groups.
Injury was defined as a musculoskeletal concern requiring medical attention as recorded on training session logs from each participant and investigated by the program leader. Injury rate/100 person- months was calculated ((total number of injuries from all participants / number of participants) / total number of days enrolled in the study (77 days x 30 days/month x 100 months)). Drop-out was defined a priori as explicit withdrawal from the study by a participant or missing three consecutive sessions.
Results
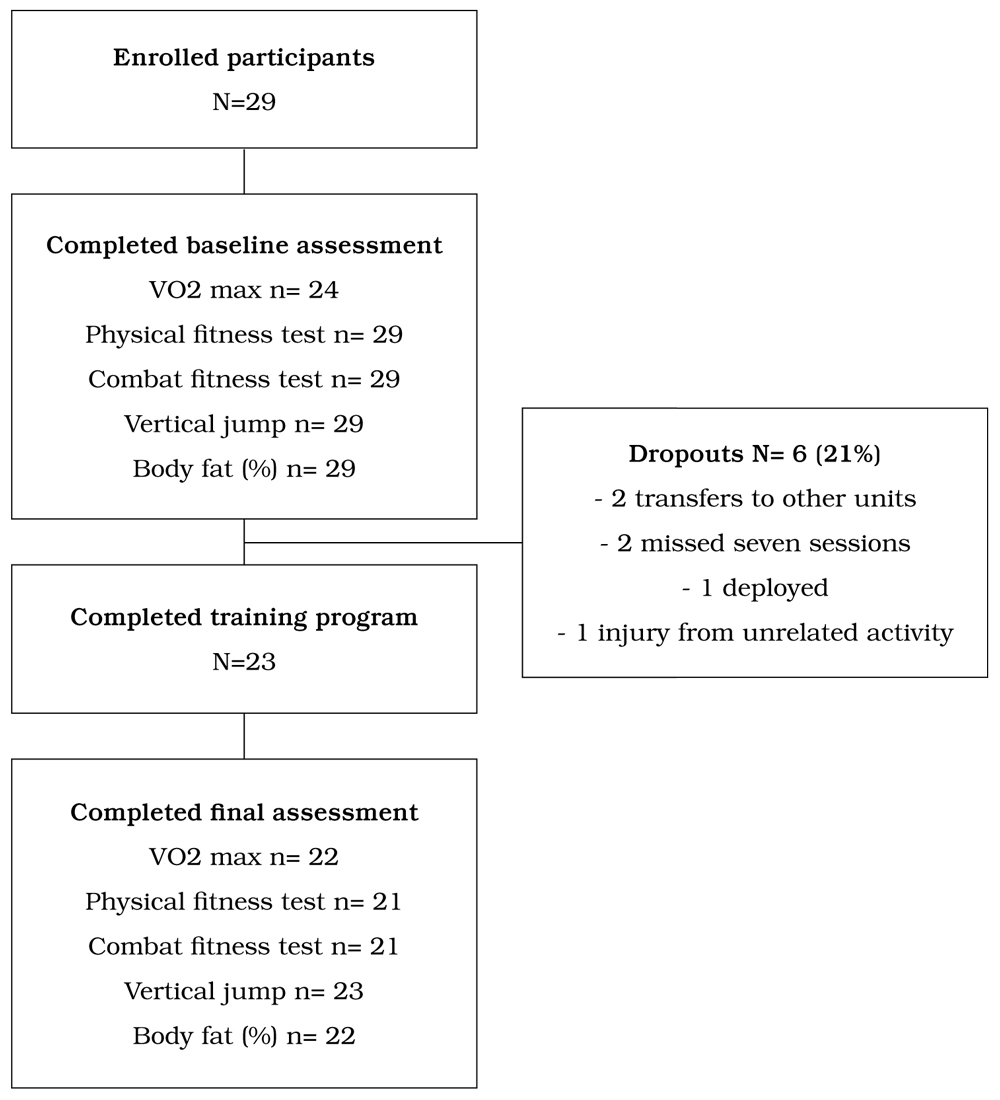
A total of 29 garrisoned US Marines were recruited and consented to participate in the 11-week CCAP. Six participants (21%) dropped out of the program – two transferred to different units, two missed seven sessions, one deployed to Afghanistan, and one broke his wrist in an activity not related to the research or fitness training (Figure 1). The sample group was comprised of 25 males and 4 females, and the mean ± SD values for age was 23.1 ± 4.4 years. The overall time in the USMC was 3.47 ± 3.52 years, meaning most study participants were nearly done with their first four-year enlistment. Only 4 (13.8%) had deployed to combat previously; 13 (44.8%) were current cigarette smokers; 12 (41.4%) were past smokers, and 4 (13.8%) were never smokers (Table 1).
Figure 1. Flow diagram of participation.
Sixteen Marines completed maximal cardiopulmonary exercise tests before and after training (Table 2). Baseline VO2 peak (49.0±10.4 ml·kg·min-1) increased by +5.3% (51.6±6.3 ml·kg·min-1) following training (p = 0.011). Similarly, VO2 at the VAT increased by +4.7% following training (Pre vs Post: 33.5±7.6 vs 35.0±4.2 ml·kg·min-1, p < 0.001). The mean increase in VO2 peak and VO2 at the VAT from pre- to post- training was 0.33±0.4 L·min-1 and 0.24±0.6 L·min-1, respectively (Figure 2).
Other measures of fitness, including PFT, CFT, vertical jump and % of body fat, all improved from baseline to endpoint. Of these, only improvement in the PFT was statistically significant in the paired-t test (p <0.05) (Table 2).
Among the entire sample (n=29), participants completed 744 training sessions, – mean 25.7 (78%) of 32 planned sessions. Among participants who did not drop out (n=23), participants completed 677 sessions – mean 29.4 (89%). A total of 79 sessions were missed (prior to drop-out among non- completers): 63 (80%) were missed due to conflicting duties; 12 (15%) due to leave or other excused absence; 2 (2.5%) due to musculoskeletal concerns; and 1 (1.3%) due to feeling tired.
Eight participants (27.6%) recorded musculoskeletal concerns in 13 (1.7%) training session log entries. Five concerns were among the moderate-intensity participants and three among the high-intensity participants: musculoskeletal concerns related to knee (4 (31%)); ankle (2 (15%)); and one report each for hamstring, shin, low back, foot/toe, calf, groin and unknown (8% each). Only one of these concerns (‘groin pull’) was associated with medical attention, meeting our a priori definition of an injury. Two entries (‘groin pull’ and ‘shin splints’) were associated with missing a training session but did not meet our criteria for injuries (Table 3). The calculated injury rate was 1.34 injuries/100 person-months.
Table 1. Characteristics of participants (by intervention group).
| Overall (n=29) | CCAP-Mod (n=16) | CCAP-High(n=13) | ||||
|---|---|---|---|---|---|---|
| Characteristic | Number | % | Number | % | Number | % |
| Sex (male) | 25 | 86.2 | 14 | 87.5 | 11 | 84.6 |
| Race | ||||||
| White | 16 | 55.2 | 10 | 62.5 | 6 | 46.2 |
| Black | 7 | 24.1 | 4 | 25 | 3 | 23.1 |
| Other | 4 | 13.8 | 2 | 12.5 | 2 | 15.4 |
| Missing | 1 | 3.4 | 0 | 0 | 1 | 7.7 |
| Ethnicity (Hispanic) | 11 | 37.9 | 5 | 31.3 | 6 | 46.2 |
| Deployed (yes) | 4 | 13.8 | 2 | 12.5 | 2 | 15.4 |
| Tobacco Use | ||||||
| Current | 13 | 44.8 | 8 | 50 | 5 | 38.5 |
| Past | 12 | 41.4 | 8 | 50 | 4 | 30.8 |
| Never | 4 | 13.8 | 0 | 0 | 4 | 30.8 |
| PCL PTSD Screen Positive (yes) | 4 | 13.8 | 2 | 12.5 | 2 | 15.4 |
| AUDIT Screen Positive (yes) | 3 | 10.3 | 0 | 0 | 3 | 23.1 |
| mean | SD | mean | SD | mean | SD | |
| Age (years) | 23.1 | 4.4 | 23.94 | 4.25 | 22.1 | 4.1 |
| Time in service (years) | 3.47 | 3.52 | 3.59 | 2.95 | 3.15 | 4.4 |
| IPAQ score (METs/week) | 4557.49 | 3740.38 | 4453.5 | 3057.4 | 5662.34 | 4607.1 |
Notes: CCAP- combat conditioning assessment program; SD- standard deviation; IPAQ- International Physical Activity Questionnaire; METs- metabolic equivalents; PCL- PTSD Checklist List; PTSD- Post-traumatic stress disorder; AUDITAlcohol Use Disorders Identification Test.
Figure 2. Pre- post-changes in physical performance measures
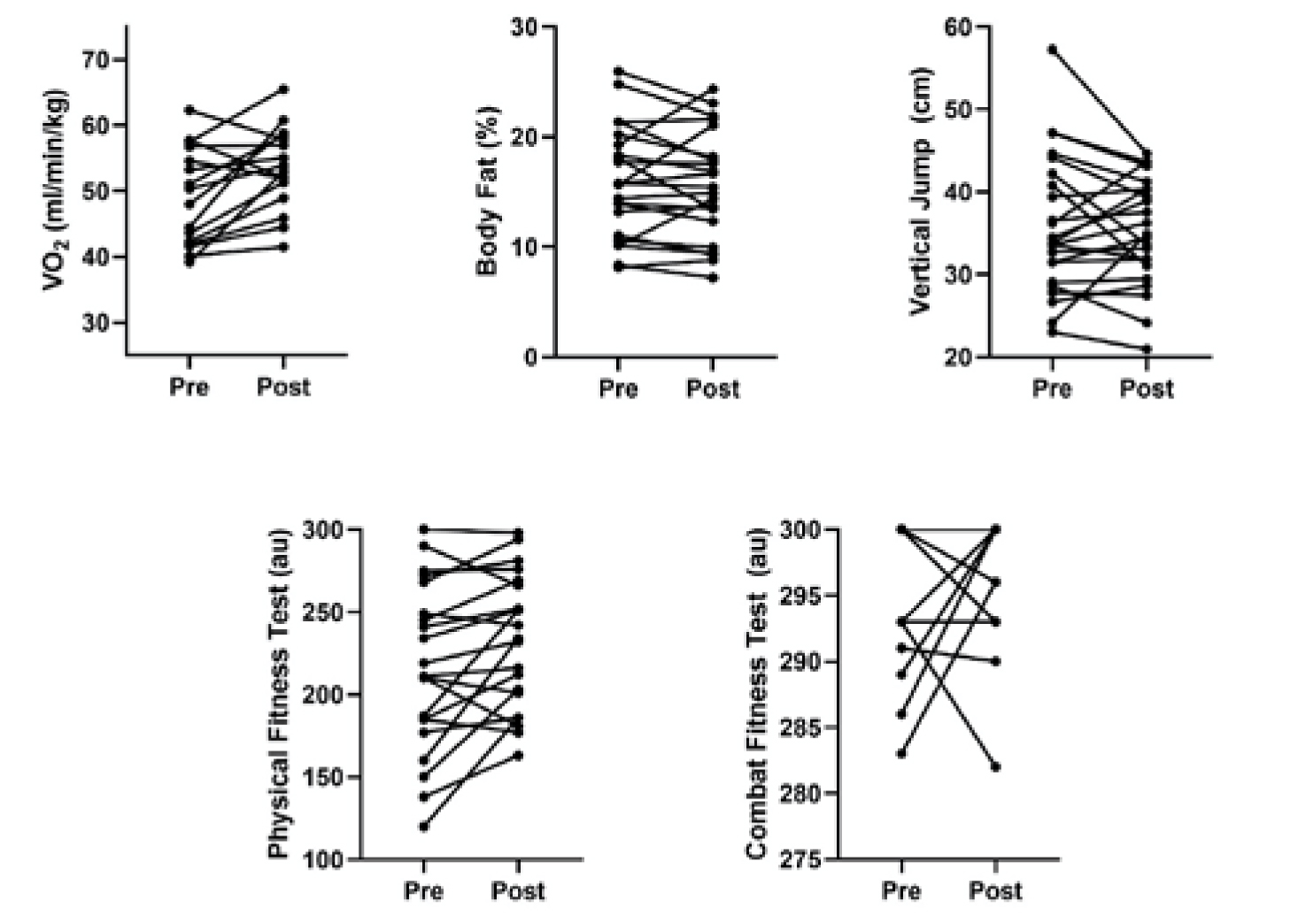
Note: Individual plots of selected for performance variables before (pre) and after (post) exercise training. The figures illustrate individual participant change in performance variables of potential value to future studies of systematic training regimens.
Table 2. Physical performance of participants (high- and moderate-intensity combined) at baseline and endpoint.
| Baseline | Endpoint | 95% CI for mean difference |
|||||||
|---|---|---|---|---|---|---|---|---|---|
| Outcome | M | SD | M | SD | n | r | t | df | |
| VO2 peak (ml/min/kg) | 49.06 | 7.37 | 53.54 | 6.30 | 16 | -7.77, -1.19 | 0.60 | -2.90* | 15 |
| Body fat (%) | 15.82 | 5.05 | 15.52 | 4.92 | 22 | -0.82, 1.42 | 0.87* | 0.55 | 21 |
| Vertical jump (cm) | 35.91 | 8.39 | 35.24 | 6.50 | 23 | -1.71, 3.40 | 0.76* | 0.58 | 22 |
| Physical fitness test score | 215.52 | 50.94 | 231.95 | 40.84 | 21 | -29.32, -3.53 | 0.83* | -2.66* | 20 |
| Compact fitness test score | 295.24 | 5.26 | 295.95 | 4.77 | 21 | -3.52, 2.09 | 0.25 | -0.53 | 20 |
*p < 0.05
Table 3. Summary of all musculoskeletal concerns (n=13) and injuries (n=1).
| Location | n | % | |
|---|---|---|---|
| Musculoskeletal | |||
| Knee | 4 | 31 | |
| Ankle | 2 | 15 | |
| Hamstring | 1 | 8 | |
| Shin | 1 | 8 | |
| Low Back | 1 | 8 | |
| Foot/toe | 1 | 8 | |
| Calf | 1 | 8 | |
| Groin | 1 | 8 | |
| Missing | 1 | 8 | |
| Musculoskeletal injury | |||
| Groin | 1 | 100 |
Discussion
As hypothesised, this pilot project supports the use of a linear periodised training program to improve cardiopulmonary fitness, with a low rate of musculoskeletal injuries. In comparison to traditional continuous training, shorter periods of interval training appear superior with respect to improving cardiorespiratory fitness (i.e., peak VO2). In fact, shorter interval-style training appears to increase VO2 peak on average 0.5 L·min1 whereas more traditional continuous style training increases VO2 peak by approximately 0.2–0.3 L·min1.18 In the present study, our training program elicited significant improvements in VO2 peak with a mean increase of 0.3 L·min-1. Previous studies have examined healthy sedentary populations; therefore, the above-average VO2 peak recorded before training (49.0±10.4 ml·kg·min-1) in our sample may have limited participants’ trainability. Moreover, our program was not designed specifically to increase cardiorespiratory fitness. Additionally, we recorded improvement in strength as demonstrated by increased counts of crunches and pull-ups. Figure 2 illustrates the individual-level changes in key measures of fitness and performance to inform future studies of systematic physical training programs.
The CCAP training program was safe with a low injury rate. Our only musculoskeletal injury occurred to a participant while running outside of the program and attribute the injury to the extra mileage volitionally undertaken by the participant. This resulted in an injury rate of 1.34 injuries/100 person-months, at the low end of published rates for garrisoned units. Non-combat MSIs have been similarly observed in all settings of military service, including basic training, garrison and deployment. For instance, during basic training, injury rates in the Army and Navy have been shown to be 6–12 per 100 male recruits per month (100 person-months), with rates rising as high as 30 per 100 per month for Naval Special Warfare training.19 Rates of MSIs are higher among women.20 Rates of injury among garrisoned infantry have been observed to be 95 injuries per 100 soldiers per year (7.9 per 100-person-months), with 50% of those injuries occurring during physical training. Another study reported that 51% of garrisoned infantry sustained an injury over six months.21 Rates of injury in the military are significantly higher than those observed in civilian populations of the same age.22 Studies have shown that some of the risk factors for sustaining injury include low baseline fitness, participation in sports, high running mileage and high weekly exercise volume.19
Decreasing musculoskeletal injuries should be a priority for the Department of Defense. While numerous studies7 acknowledge the problems created by the military’s unstructured fitness program, changes have mostly been incremental (e.g., reduced running mileage, modifications to footwear) rather than shifting to a more modern, evidence-based paradigm that incorporates modern physiology and exercise science principles. One attempt at an overhaul was the Army’s Physical Readiness Training during advanced infantry training. The program incorporated progressive and individualised overload as well as injury control education that resulted in both reduced injury occurrence and time loss from injury.21 This program’s preliminary success demonstrated the likely benefits of a systematic approach and the need to evaluate the broader implementation of linear periodised training programs.
Feasibility of a more structured training program is critical. Military units train in a variety of locations/ settings, and often do not have a lot of equipment for physical training. In addition to formal physical training, service members are regularly assigned to non-fitness activities that are physically demanding. Marines and other military personnel have tasks such as rifle range training, work details that arise with little notice, or training changes to alternative locations. Our data indicated that these other duties contributed to 80% of the missed sessions and showed that they take priority over fitness training. Disruptions like these can affect the effectiveness of a training program; although, in this pilot, some measures of fitness demonstrated improvement despite these disruptions. Attributes of the program to address missed sessions including careful documentation of the reason for missing, rescheduling sessions +/- one day, and close supervision of adherence may be necessary to maintain the fitness benefits. Training programs based on linear periodisation must factor in such disruptions and mitigate them to the extent possible.
This study provided proof of concept that properly trained active-duty Marines can improve their fitness, with a low injury rate, while still participating in other critical assignments. While we did not explicitly assess cost, the program was administered by a single program leader, trained as a strength and conditioning coach, who could be utilised by several units or monitor a group larger than 30 individuals. Unit commanders can apply similar programs to their units to increase physical fitness. This program would likely need to be adapted to serve units of different types or in a different phase of the deployment cycle and may involve more sophisticated periodisation strategies, such as block periodisation.
A weakness of the study is that the sample was small and recruited from a single unit; although this allowed for very close supervision and maximised interaction by the program leader. Larger groups should be studied to see if the same results will occur without this intimate level of guidance and oversight. We were also unable to follow up with the cohort beyond the completion of the training program. Thus, the sustainability of this approach without supervision or the maintenance of the observed fitness benefits is unknown. Incomplete data also limit the internal validity of our performance and fitness findings. For example, various challenges, including power outages at the time of testing, inability to schedule testing for a participant, participant drop-out and poor-quality data limited the number of participants with pre- and post-maximal exercise data to 16. For these reasons, the purpose of the study evolved after it was in the field and the focus shifted to assessing feasibility and informing future projects. In future research, a more considerable effort may be required to enhance complete data collection.
Conclusion
Our findings provide evidence of the feasibility, safety and physical performance and fitness benefit of a systematic approach to physical training of a garrisoned military unit. The USMC and other branches of the US military should build on studies such as this one and further assess a linear periodised training program and assess improvements in fitness and injury rates.
Corresponding Author: Drew Helmer drew.helmer@va.gov
Authors: C Heard1, M Willcox2, M Falvo3,4, M Blatt5, D Helmer3,4
Author Affiliations:
1 Protac
2 US Army Medical Department
3 Department of Veterans Affairs
4 War Related Illness and Injury Study Center
5 Hackensack University Medical Center