
Introduction
The First World War produced a range of combat- related injuries that severely challenged the resources and technical abilities of medical services at the time. The surgical sub-specialties that evolved in response to this “new age” of warfare included thoracic surgery, orthopaedic surgery, neurosurgery and plastic/maxillofacial surgery.1,2. Units specialising in face and jaw surgery, as it was known then, typically comprised of a plastic surgeon, a dental surgeon and a dental technician and the close relationship between these areas of expertise reflected the complex and challenging nature of managing such injuries. Fractures of the mandible were managed primarily with intraoral appliances utilising the existing dentition to stabilise the fracture segments once occlusal reduction had been achieved. Such appliances were also used to treat continuity defects of the mandible allowing the correct anatomical relationship to be maintained between treatment episodes and preventing wound contracture.
Fractures of the midfacial skeleton were more problematic due to the relatively primitive state of diagnostic imaging and the limited means to anatomically reduce the fractures and provide rigid fixation for healing. There were also concerns in surgically exposing such fractures and the perceived risk of infection. We present a unique historical illustration of the use of a traction device utilising an intraoral appliance and distraction screws to correct a midfacial deformity resulting from a combat related injury.
History and Examination Findings
Soldier WC (aged mid-twenties) sustained a perforating gunshot wound through both cheeks and a shrapnel (sic.) wound to the right cheek in February 1917.3 WC was admitted under the NZ section (Major HP Pickerill, OC) at the Queen’s Hospital in Sidcup in November 1917 and his examination findings at that time were summarised as follows: “…the whole of the upper face had fallen backwards, the nose was sunken and depressed, the maxilla was too far back by three quarters of an inch, as judged by the hiatus between upper and lower teeth, zygomas had united but were in malposition and bulging outwards; there was also a long scar and an unsightly swelling on the right cheek”.4 It was also noted that WC was deaf in the right ear, had lost most of the sight from his right eye and was in a septic condition. No attempt had been made to control the facial fractures.
Due to his poor general condition extensive surgery was deferred and the decision was made to correct the facial fractures using a dental appliance instead, which could be used as a traction device to bring the fracture segments into better anatomical alignment. It is unclear from the case notes if the fracture sites were opened surgically but the maxilla was “reset” and brought forward in order to re-establish premorbid dental occlusion and reduce the acquired antero-posterior discrepancy between the maxilla and mandible. The patient wore this traction appliance for approximately six months after which the appliance was removed and the maxilla immobilised against the mandible using double gunning splints3. Minor surgeries to correct nasal bone projection and scar revision were performed during the period of bony healing and by December 1918 the splints were removed. Pickerill reported that the patient was able to eat a regular diet and there was an overall improvement in his psychosocial condition.
The Traction Appliance
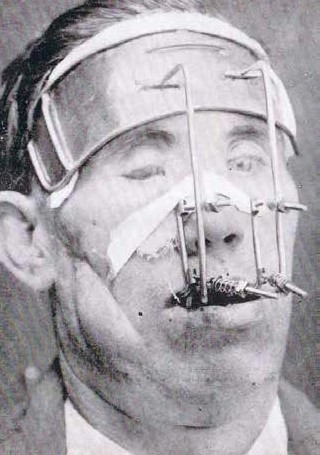
Figure 1. Photograph of the patient and traction appliance in situ (original photograph quality is poor).

Figure 2. Photograph showing the dental traction appliance with spring mechanisms and threaded screws. The craftsmanship involved in making such a device is particularly noteworthy.
Pickerill pays a rare tribute to the expertise of his dental surgeon colleague Major Rishworth, who along with Captain Turner (NZ Dental Corps), provided the fracture management of this patient. The appliance itself consisted of cast splints which were cemented onto the upper and lower dentition. The maxillary splint had a pair of short vertical arms that extended outwards on either side of the nose, while the mandibular splint had two longer arms extending up to a metal plate which rested onto the forehead and secured by bandages (Figure 1). The maxilla was gradually pulled forward by tightening a set of screws which were spring loaded to give slight tension during the distraction of the maxilla. The screws could be replaced over time as the length of the threads became too short and this was accomplished by simply removing the threaded screw by means of a housing into which the head of the screw was slotted (Figure 2). The technical expertise, innovative design and art can be fully appreciated when the appliance is closely examined.
Discussion
This patient exemplified the problems of casualties with facial fractures presenting late to face and jaw units. This may have been due to a number of factors including the tactical environment, delays in medical evacuation, poor general condition of the patient and a lack of appreciation of the surgical needs of the patient.
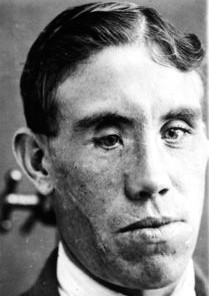
Figure 3.Late post-operative photograph of patient showing improved maxillary position and scar revision. Residual enophthalmos of the right eye remains.
The pattern of injury of this patient highlights the difficulty in managing midfacial injuries at a time when open reduction and internal fixation was not possible. The only possibility given the poor general state of the patient was to gradually distract the fractures using a dental appliance and what Pickerill termed an “orthodontic” method4 but what would now be considered as dentofacial orthopaedics. Pickerill was qualified in both dentistry and medicine and possessed a better appreciation of orthodontic principles than some of his surgical colleagues. The innovative use of an external traction device combined with an intraoral appliance is of particular significance as the concept of gradually moving separate bony segments into position over time using a screw-traction appliance has been reincarnated for craniomaxillofacial use today in the guise of distraction osteogenesis devices for the surgical management of congenital craniofacial deformities. Figure 3 shows a post-treatment photograph with a general improvement in facial appearance. There is still a degree of right enophthalmos and an impression of a flattened midface but given the limited treatment options at the time, the results are very satisfactory. Presenting historical case material is often difficult due to incomplete or missing background information. However, this case study presents a rare combination of written notes, photographs and archival material – in this case the appliance itself.



