
Abstract:
Alcohol was widely believed to induce malaria recurrence in the early 20th century, but no physiological mechanism was recognised. Allied military units during World War II experienced vast numbers of malaria infections without any obvious reported overlap with alcohol ingestion. Historical and recent reports of malaria’s relationship to alcohol have been reviewed and found inconclusive. It is most likely that social factors associated with chronic ethanol use, such as late-night, outdoor activities, promoted mosquito exposure and parasite infection. Relapsing malaria (Plasmodium vivax) was very common in soldiers in the Southwest Pacific theatre. However, there is no substantial evidence that binge drinking promotes relapses of latent parasites from the liver. Alcohol’s association with malaria is likely due to sociology and not pharmacology.
Keywords: malaria, alcohol, military, World War II
The explanation of these cases appears to be that the subtertian malaria infection is lying latent until aroused into activity by the exposure to cold, alcohol or some other factor.1 – Philip Manson-Bahr, 1926
Alcohol was widely believed to induce malaria attacks as described in the classical tropical medicine texts; an example is shown above from a century ago. It is easy to see how such beliefs arose, given the stereotype of the colonial-era, alcoholic expatriate plantation owner in Africa, taking intermittent quinine doses between his whiskey shots. In my own experience in East Africa, it was the town drunkards who first became malaria positive during malaria prevention trials, suggesting that there was some factual basis for alcohol-induced malaria reoccurrence.2 Mosquitoes may be more attracted to those consuming beer.3 Malaria parasites must go through a developmental stage in the liver, implying that a hepatotoxic drug like alcohol might have a role in reoccurrences from the liver (relapses) as opposed to resurgences from the blood (recrudescences). The factual basis for alcohol-induced malaria reoccurrences during World War II is reviewed here and found wanting. Social factors associated with alcohol use may be a better explanation for apparently increased malaria rates in chronic users of ethanol rather than any pharmacological effect on the parasite in the blood or liver.
Even before the mosquito vector of malaria was discovered, the US Army associated malaria and alcohol use. An epidemic of malaria occurred in US soldiers stationed at Washington Barracks and Fort Myer in Washington, DC, in 1896 along the Potomac River.4 MAJ Walter Reed, who later discovered that mosquitoes spread yellow fever, was called to conduct an epidemiological investigation, which did not confirm the locally accepted understanding that malaria was due to a defective water supply at Washington Barracks. Reed’s opinion was that the soldiers were getting infected with malaria while travelling from their barracks at night through the Potomac swamplands to reach the saloons of Washington. This was especially true of those so inebriated by alcohol that they collapsed on their return journey and slept in the swamps among the mosquitoes.4 Reed did not figure out that it was the mosquitoes that spread malaria, but he came close by eliminating water but not ethanol ingestion as the cause of the epidemic.
Malaria can recur either as a recrudescence of an existing blood infection, usually Plasmodium falciparum or as a relapse of a latent hepatic infection, usually P. vivax. Most of what seemed to be discussed as an alcoholic predisposition to increased malaria in the colonial era appears to be the former case, with alcohol causing more clinical attacks of existing malaria infections. Intemperate habits were often linked to alcohol use in expatriate administrators and soldiers scattered widely across isolated tropical postings. Since the only effective medication for malaria in the early 20th century was quinine, which had to be taken as a daily suppressive dose, any hangover-induced interruption in such a demanding routine was likely to result in a febrile attack.5 One colonial adaptation of quinine was to put the drug into ‘bitters’ as flavouring and mix it with the gin. Intermittent quinine use was linked to blackwater fever, a still poorly understood consequence of imperfectly suppressed falciparum infections.6 The role of alcohol was uncertain at best, as there was never enough quinine in the bitters of gin and tonic to constitute an effective dosage against parasites, despite the belief by no less a person than Winston Churchill that the tonic given with gin had saved many lives in the British Empire.7 It seems most likely that malaria and alcohol were coincident factors in colonial governments and militaries’ approach to living in the tropics, regardless of any medical connections between the two factors.
Alcoholics are more susceptible to malaria than the temperate, and in them malaria is more severe.8 – Patrick Hehir, 1927
Allied armies were particularly challenged by malaria infections during World War II, particularly in soldiers deployed in Africa, India and the Pacific Islands. Malaria casualties were of utmost concern in the Southwest Pacific theatre as entire infantry divisions required months after deployment on Pacific Islands to rehabilitate in non-malarious areas during multiple bouts of relapsing malaria.9 The extraordinary frequency of malaria relapses, often exceeding 10 in a single soldier, raised questions about why this was so different from prewar medical experience. Although imperfect chemosuppression, frequency of infection and wartime conditions likely explained much of the increased malaria incidence, there were attempts to blame the victim.10 Alcoholic excess has been blamed as the cause of many soldiers’ shortcomings, including malaria, especially when the analogy from the drunken colonial plantation owner was carried over into the military.
However, the logistical problems created by distances in the Indo-Pacific Region made alcohol a difficult-to-obtain commodity for most military members. Unlike the British Royal Navy, which continued its daily issue of diluted rum (grog) to its sailors, or the French Army, which gave each soldier half a litre per day of vin ordinaire, most Allied soldiers had only episodic exposure to alcohol, usually when on leave and rarely any at all during combat operations.11 Those with access to superior transportation assets such as the Air Forces often found creative means to obtain alcohol over long distance supply lines. See Figure 1. Medicinal ethanol was distinctly limited and was supposed to be issued only by medical units. Limitations on sources of ethanol in the Pacific region were often so severe that sailors resorted to locally devised distilleries of fermented sugar (so-called raisin-jack) and citrus juice mixed into torpedo fuel (so-called torpedo juice) before the quartermasters diluted it with poisonous methanol.11 Certainly, soldiers on leave in Australia during World War II had greater access to alcohol than in New Guinea and used it freely, as noted in civil disturbances fuelled by alcohol, such as in the ‘battle of Brisbane’.12
Figure 1: Two RAAF airmen drinking beer in Morotai, Halmahera Islands, Netherlands, East Indies (now Indonesia) in March 1945. Photo AWM OG2308 by John T. Harrison, now in the public domain.
But did alcohol have any causative relationship with the extraordinary numbers of P. vivax relapses encountered in the Allied Armies in the Pacific during World War II? Binge drinking would seem to be the most likely situation in which malaria relapses could have been induced, and the intermittent supply of alcohol certainly promoted such behaviour.13 There are significant problems trying to relate an individual’s behaviour with alcohol to malaria relapses in large military populations, primarily due to lapses in chemosuppression with mepacrine (atabrine). Enforced military compliance with daily mepacrine was effective in stopping malaria casualties but was also resented by soldiers who would often omit taking daily medication while on leave. Chemosuppression, indiscipline or non-compliance may have been linked to hopes that a malaria relapse might prolong one’s leave period and thus limit exposure to combat conditions back in the jungle. Fairley best described the epidemiology of malaria in the Australian Army and shows 1943 and 1945 epidemic peaks overseas (mainly in New Guinea) with echo increases afterwards in Queensland, as seen in Figure 2.14 The 1944 peak of malaria in Queensland was almost entirely due to P. vivax relapses from soldiers returned from New Guinea and was most likely due to withdrawal of mepacrine chemosuppression.15 There is no direct way to relate malaria relapses in Queensland to increased access to alcohol compared to combat operations in New Guinea. However, it cannot be ruled out for some individuals.
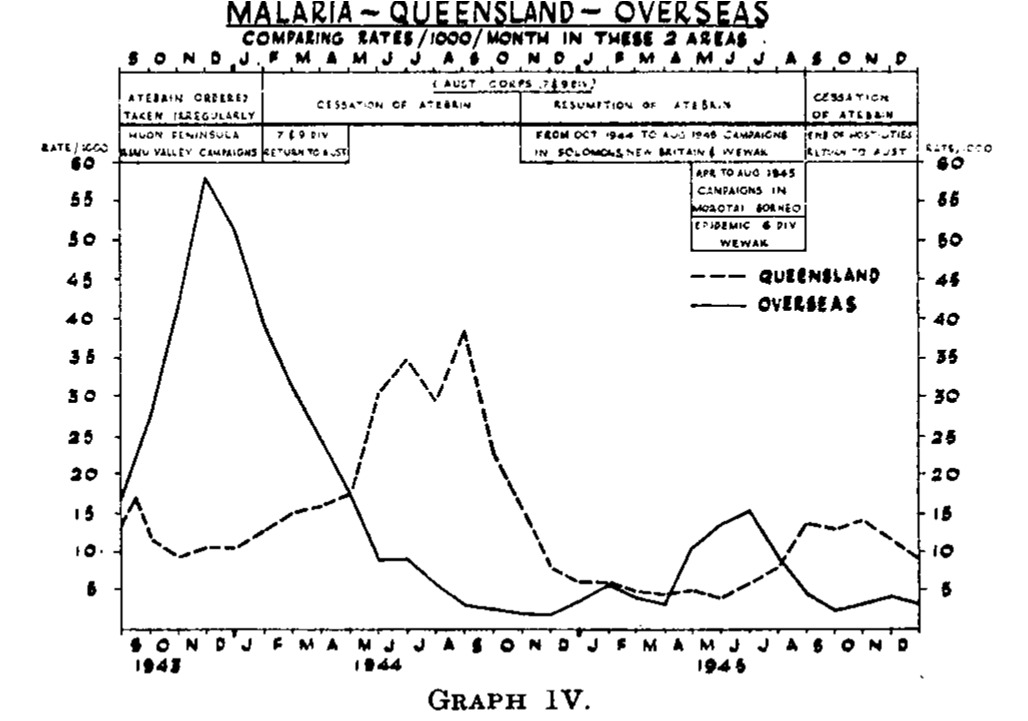
Figure 2: Malaria in Australian Army Soldiers in Queensland and Overseas (mainly New Guinea) during World War II, 1943–45. Note the dotted lines showing secondary peaks of relapsing malaria, largely occurring in Queensland following overseas malaria (solid line). Access to alcohol in Australia was much greater than overseas. However, the explanation for the secondary peaks in Queensland is more likely to be discontinuation of suppressive drug prophylaxis.14 Reproduced from Medical Journal of Australia 1946.
An analogous situation existed with the US Army fighting in North Africa and Italy. By 1945, many soldiers still had residual parasites in their livers from previous infections, which were largely suppressed by daily mepacrine as the war moved further north into Europe. Alcohol was certainly more available in Europe than in the Pacific Theater. This was particularly true when the armed conflict ended in May 1945. The end of World War II in Europe resulted in much Allied rejoicing and alcohol bingeing. Many US soldiers did not remember much about the Victory in Europe (VE) celebrations other than the huge hangover afterwards. Figure 3 shows the overall malaria epidemiology for the Mediterranean Theater for the US Army.16 There is no evidence of any increase in malaria associated with VE Day, but neither was there any removal of chemosuppression as had occurred in Australia. Therefore, there is no population-based data to indicate that alcohol ingestion promoted P. vivax relapse in either the Australian or US Armies of World War II. However, the data are insufficiently granular to rule out such an effect in some individuals.
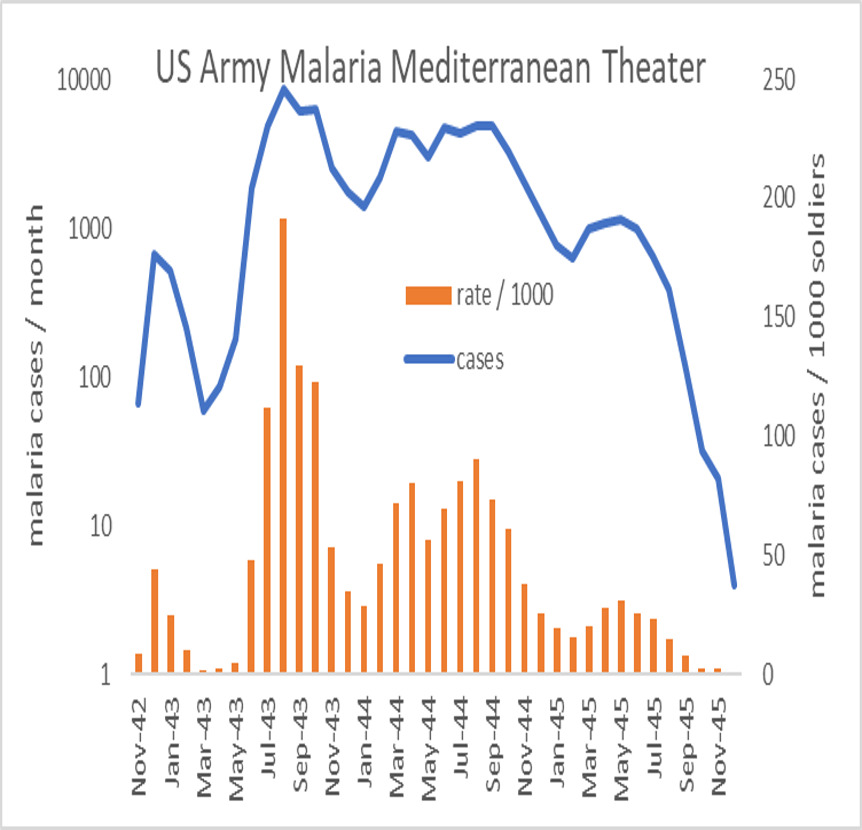
Figure 3: Adaptation of epidemiological observations of malaria in the US Army in the Mediterranean theatre taken from the Official Medical History of the US Army in the Second World War.16,18 Note that Victory in Europe (VE) Day occurred on 8 May 1945 and was accompanied by a great deal of celebratory binge drinking. No upward change in malaria incidence was noted in 1945, but suppressive medications were not formally discontinued until soldiers returned to the USA. Note that malaria cases on the left axis are on a logarithmic scale.
It is reasonable to think that a hepatotoxic drug such as ethanol might affect a parasite like malaria, which undergoes an obligatory hepatic phase after inoculation by mosquito. There are many associations of alcohol and the tropics, which may share some overlap with malaria. The problem is seeing whether these associations have any causative value. Despite long traditions, such as gin and tonic, the tropical myths about what does and does not promote malaria largely remain in the category of mythology.7 Binge drinking in soldiers is important but has only been seriously studied recently.13 Alcoholism was not really considered in the entire 20-volume British Official Medical History of World War II, despite its extensive details on malaria.11 Social observations combining alcohol and malaria are common, but it appears to be mostly coincidental. Walter Reed’s observation that the drunken soldiers were the ones who got malaria was correct. However, the connection was the mosquitoes in the swamps around Washington, not the ethanol in the saloons.4 Chemotherapy remains the basis of most malaria control in the military. Military malaria is often presented as a management problem associated with discipline and medication compliance.17 Wartime epidemics of P. vivax malaria in Queensland and Italy centred on the use of mepacrine, not ethanol.14,16 Therefore, it is fine to enjoy tonic water in your gin in moderation, but do not expect the quinine in the bitters to protect you from malaria or the gin to induce a relapse.
Author affiliations: Australian Defence Force Infectious Disease and Malaria Institute, Gallipoli Barracks, Enoggera, Queensland, Australia
University of Queensland, School of Public Health, Brisbane, Herston, Queensland, Australia
Funding: No specific funding was given for this work. The author is an employee of the Australian Defence Force, a retired US Army officer and claims no conflicts of interest.
Disclaimer: The opinions expressed are those of the author and do not necessarily reflect those of the Australian Defence Force or the US Department of Defence.
Please specify the URL of your file



