
ABSTRACT:
Background: The Functional Movement Screen is a tool used in athletic populations for predicting injury potential by assessing movement dysfunction. This tool may be of use in tactical populations (police officers, firefighters and military personnel) who perform daily duties of a physical nature, often carrying loads that negatively affect their movement patterns and cause physical injury.
Purpose: This purpose of this review was to explore the literature on the use of the Functional Movement Screen in tactical populations.
Methods: Literature databases were searched using key search words and terms. Studies meeting the inclusion criteria were critically evaluated using the Downs and Black protocol. Inter-rater agreement was determined by Cohen’s Kappa.
Results: Five articles were retained for evaluation with a mean Downs and Black score of 73%, (k=0.82). Studies included both genders from military and firefighting populations.
Conclusion: Research suggests that the Functional Movement Screen can be reliably applied to a tactical population and may be of use as a screening tool. A score of below 14 may indicate an increased risk of injury. Furthermore, the tool can be used to evaluate the effectiveness of tactical conditioning programs. Further research is required to confirm and advance these findings within this population.
KEYWORDS
Functional Movement Screen, military, solider, tactical, injury
INTRODUCTION
Tactical personnel, who include police officers, firefighters and military personnel, are required to wear external loads while performing daily duties. These loads, which are determined by daily duty requirements, consist of items like protective body armour and personal weapons. For the general duties police officer these loads could equate to 10kg and for the specialist police up to 27 kg1,2, while for the firefighter a standard load of protective clothing, breathing apparatus and specific tools can equate to 37kg3. For the average military rifleman a fighting load of around 29 kg and marching order load of over 50kg is not uncommon4,5. The duties performed while bearing these loads can include tasks that require the performance of dynamic movements (running, jumping, crawling, balancing, climbing, lifting, carrying, pushing, pulling, fighting and dragging) over dynamic environments (rugged and harsh terrains)1,4-6. As such, the addition of external loads can affect tactical personnel in a number of ways, from reducing their physiological function4, task performance7 and ability to tolerate heat8, to increasing their energy expenditure while performing a given task9. In addition, carriage of external loads is known to impair balance6, change gait patterns (running and walking) 6,9,10, influence postural stability4,6 and is associated with an earlier onset of muscle fatigue6,9.
Given the nature of their duties, which can impart significant physical stress over prolonged or repeated periods1 and noting the influences of carrying external loads, it is not surprising that load carriage is associated with causing musculoskeletal injuries [acute and overuse injuries] to tactical personnel11-13. Musculoskeletal injuries cause a reduction in physical performance, training and duty time, morale and operational readiness while increasing medical and training costs12,14,15. Chronic conditions, which could present if musculoskeletal injuries are not identified early, can preclude soldiers from completing training16 or returning to duty17 and are associated with reductions in operational readiness12.
One means of identifying the potential risk of musculoskeletal injury is through the use of the Functional Movement Screen (FMS) tool. The FMS is an evaluation tool used to assess the fundamental movement patterns of an individual in a dynamic and functional capacity18. The FMS consists of seven movement patterns that include an overhead squat, hurdle step, lunge, shoulder mobility, active straight leg raise, push-up, and rotary stability test18. To successfully complete these movements, the participant requires elements of muscle strength, flexibility, range of motion, coordination, balance, and proprioception18; elements which, when lacking, are associated with an increased risk of musculoskeletal injury19. As such, the FMS assessment tool offers an approach to injury prevention by identifying an individual’s functional limitations and / or asymmetries10,18,20,21. It is for this reason that the FMS is widely employed within athletic and physically active populations18.
With a total possible score of 21, previous studies have suggested that low FMS scores of <14 have an association with musculoskeletal injuries in athletic and general populations20-22. Kiesel et al.21 concluded that NFL players with FMS scores <14 had an 11-fold increase in the chance of injury in comparison with players with scores >14. Chorba et al.23 also concluded that female collegiate athletes who scored <14 had a four-fold increase in the risk of lower extremity injury when participating in autumn l and winter sports. Schneiders et al.22 and Perry et al.10 both confirmed that a FMS score of <14 indicated an increased risk of injury within general populations.
With the widespread use of the FMS used within the athletic population as a predictor of injury21,23, proposing its use within a tactical population is a viable concept. If the FMS can be reliably and validly employed in the tactical population, its implementation could inform strategies to reduce musculoskeletal injuries (and their associated costs) to both the individual and their unit. The aim of this review was to critically explore the literature on the effectiveness of the FMS within a tactical population.
METHODS
Keywords and terms were entered into the search engines of five literature databases and were manipulated to suit the search capabilities applicable of each database. The databases searched and keywords and terms used are outlined in Table 1.
| Data Base | Search Term | Filter | Number after inclusion | Number after exclusion | Duplicate | New articles |
| CINAHL |
Functional movement screen AND military OR soldiers Functional movement screen AND military Functional movement screen AND soldiers “Functional movement screen” AND military OR soldiers |
2003-2013, English, Humans |
8 | 2 | 1 | 1 |
| PubMed |
Functional movement screen AND military OR soldiers Functional movement screen AND soldiers Functional movement screen AND military “Functional movement screen” AND military OR soldiers “Functional movement screen” AND military |
2003-2013, English, Humans, Adult 19+, core clinical journal articles |
5 | 2 | 1 | 1 |
| Pro Quest |
Functional movement screen AND military OR soldiers Functional movement screen AND military Functional movement screen AND soldiers “Functional movement screen” AND military OR soldiers |
0 | 0 | 0 | 0 | |
|
Pro Quest (Military)
|
“Functional movement screen” AND military OR soldiers “Functional movement screen” AND tactical population |
3 | 0 | 0 | 0 | |
| Medline |
Functional movement screen AND military OR soldiers Functional movement screen AND military Functional movement screen AND soldiers “Functional movement screen” AND military OR soldiers |
5 | 1 | 2 | 2 |
Table 1: Details of literature search: database used, search terms and inclusion filters
After collection of all preliminary articles, duplicates were excluded and abstracts were subjected to specific inclusion criteria. The inclusion criteria comprised of: a) the study being published in the English language, b) the study being published within the last decade, and c) the study involving both the FMS and human participants. Once identified, the collected articles were then subjected to specific exclusion criteria to remove literature not relevant to this paper. These exclusion criteria are shown in Table 2.
|
Studies were excluded if the they included; a) the use of devices that alters movement (i.e. strapping tape); b) populations did not include tactical personnel (i.e. solders, first responders, fire fighters police); c) participants outside the age of typical tactical population service age (17-55yrs); d) the use of supplements (vitamins); e) a commercial interest (a certain brand of equipment); or focused on a specific piece of equipment (mountain carriage stretches); f) medically unfit (soldiers with injuries or obese subjects); g) literature not published in English and not able to be translated by software or linguistic support available to the researcher (Dutch, Spanish, French and German); h) a psychology focus (i.e. trauma; PTS; traumatic brain injury); i) only an abstract printed in journals without full text. |
Table 2: Search exclusion criteria.
While excluded, some articles were used to enrich background information and context. Once all articles were appraised against inclusion and exclusion criteria, the reference list of these remaining articles were reviewed for further potential articles as part of a secondary search process.
The included articles were critically appraised to assess their quality through use of the Downs and Black protocol24. The protocol comprises of a checklist that permits evaluation of both randomised and non-randomised studies of health care interventions24. The checklist comprises of five subcategories: reporting quality, external validity, internal validity (bias), internal validity (confounding) and statistical power. There are 27items on the checklist, for which each item is scored on a scale of ‘yes’ (one point), ‘no’ or ‘unable to determine’ (zero points). There are two additional questions with greater scoring power; Item 5 within the reporting subcategory can be scored from zero to two points, with one point given for ‘partially’ detailing confounds and two points for conclusively detailing confounds, and Item 27 within the power subcategory can be scored from zero to five points based on the sample size with a larger sample size awarded more points. The scores for each article were converted to a percentage by dividing each total score by 32 (total possible score) and then multiplying by 100. All studies were independently rated by the two authors (CB, RO) with the level of agreement measured using a Cohen’s Kappa (k) analysis of all raw scores (27 scores per paper). For final scores, any disagreements in points awarded were settled by consensus.
The total raw scores of articles following the Downs and Black checklist24 were compared to the graded system proposed by Kennelly25 to provide further validation on the quality of the articles used for this review. Kennelly25 proposed that a total Downs and Black score greater than or equal to 20 is considered a good study, between 15 and 19 is considered a fair study and scores of 14 and below is considered a poor quality study.
RESULTS
The principal search identified a total of 21 potential articles for review (see Figure 1.). A further six articles were then identified after the secondary search, with a total of 27 articles identified for review. Subsequently 22 articles were excluded as duplications or based on the exclusion criteria. Consequently a total of five articles were retained for evaluation19,26-29.
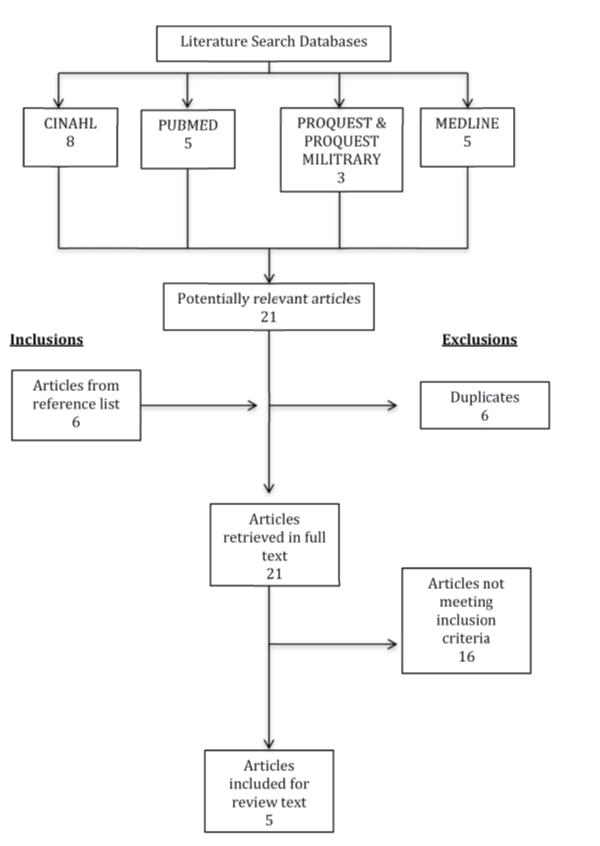
Figure 1 – FMS in Tact POP
Table 3 highlights the methods, main findings and critical appraisal quality scores for each included article. The methodological quality scores ranged from 65%26 to 78%27 with a mean score of 73%. The kappa statistic for inter-tester agreement of the methodological quality of the studies indicated an ‘almost perfect’ agreement (k=0.819)30. Based on a mean total raw score of 23.4 points the articles are generally of a ‘good’ quality when viewed through the lens of the grading system proposed by Kennelly25. The most noted limitation of these studies based on the Downs and Black protocol24 was the lack of methodological evidence regarding the blinding of participants and randomising of the groups with only one study27 meeting these criteria.
|
Author Year Title |
Participants | Study Design | Outcome measure | Measurement intervals | Results | Critical Appraisal Score |
| Frost et al.2012 “Using the Functional Movement Screen(TM) to Evaluate the Effectiveness of Training.” |
60 firefighters from Pensacola Fire Department volunteered to participate.Male only participantsParticipants were free of musculoskeletal injury or pain at the time of testing and were on full active duty.3 groups. | Cohort study The participants were assigned to 1 of 3 groups: intervention 1, intervention 2, or control.The 2 intervention groups received three 1.5-hour training sessions each week and differed in the emphasis that was placed on movement quality. |
FMS:- Individuals were graded on how they chose to perform rather than how they could perform.-Sagittal and frontal plane videos were used to grade the FMS with 3 methods-Baseline FMS above and below 13. | FMS scores were examined before and after 12 weeks of training. | The total number of asymmetries present before and after training was found to be just as variable as the individual screen scores, there were no differences between groups (p = 0.528). 85% of the participants in the control group actually changed irrespective of the baseline score.The distribution of total FMS score changes (e.g., number of increases) was dependent on the grade of the initial screen (p = 0.008). Seventeen of the 26 participants exhibiting an increase were given an initial grade <13, whereas 14 of the 17 who received a lower total post training score had a baseline FMS >13. There were no differences in the distribution of scores between groups (p = 0.653). |
72% |
| Goss et al.2009 “Functional training program bridges rehabilitation and return to duty.” |
90 Special Operations Soldiers80 males and 10 females.The mean age of participants was 35 yrs.2 types of participants stated:(1) Participation is 100% voluntary, but patients who were about to be discharged from physical therapy following extensive rehabilitation are strongly encouraged to participate.(2) Other participants are healthy individuals who have not been patients in the clinic. | Cohort study Effectiveness of a Functional training program (FTP). (The FTP is designed to prepare them for returning to full duty, resuming airborne jump status, and deployment to combat zones.)Each FTP cohort meets 3 times per week for six weeks in duration. Classes are 75 minutes in duration to include warm-up and cool down. |
FMS Other fitness test:-T-test (agility), 6 meter hop for time, single leg hop for distance, vertical jump, skin-fold body fat measure, balance test and core strength (kip-ups). |
Testing of the FMS, and fitness test conducted pre and post 6 weeks of training program. | Post functional training program FMS scores improved an average of 2.5 points. Fitness test: T-test improvement was 0.5 seconds. Single leg hop time improved 10%. Hop for distance improved approximately 10%. Body fat improvement was statistically significant. Kip-ups improved 32%. Vertical jump height improvement was statistically significant.All subjective fitness category self-evaluations demonstrated statistically significant improvements, except for pain. |
65% |
| Lisman et al.2013 “Functional Movement Screen and Aerobic Fitness Predict Injuries in Military Training.” |
874 Marine Officer Candidates Male only participants Age range = 18-30yr old 2 training groups:-6 wk (n = 447)-10 wk (n = 427) |
Cohort study 2 training groups-6 wk-10 wk |
-Exercise history questionnaire-FMS-Standardized Physical Fitness Test (PFT) (pull-ups, abdominal crunch, and 3-mile run)-Injury data were gathered | -Completed an exercise history questionnaire-Underwent FMS during medical in-processing-Standardized Physical Fitness Test (PFT) within 1 wk of training-Injury data were gathered throughout training from medical records and classified into overuse, traumatic, and any injury. | Three-mile run time (RT) was the only PFT component predictive of injury: candidates with RT >20.5 min were 1.7 times (95% confidence interval = 1.29–2.31, P G 0.001) more likely to experience an injury compared with those with RT <20.5 min. Combining slow RT (>20.5 min) and low FMS scores (<14) increased the predictive value across all injury classifications: candidates scoring poorly on both tests were 4.2 times more likely to experience an injury. |
75% |
| O’Connor et al. 2011 “Functional Movement Screen: Predicting Injuries in Officer Candidates.” |
874 Marine Officer Candidates Male only participants Age range = 18-30 years old 2 training groups:-6wk short cycle(n = 447)-10wk long cycle(n = 427) |
Cohort study 2 training groups:-6wk short cycle-10wk long cycle *Both groups have comparable training intensities and volumes withCandidates expected to be extremely fit for successful participation. |
-FMS-Physical Fitness score-Injuries Data collection-Questionnaire Data (Survey of age, tobacco use, exercise history and prior injury were incorporated into the medical screening). | -FMS-Fitness test within 1 week of starting the training program.-Data in injuries were collected daily during the training cycle. | Injury data:- Long cycle group had significant higher cumulative injury incidences for any, overuse, traumatic and serious injury-When the groups were compared as a function of injuries per 1000 person-days, the short cycle had higher incidence rates for any and traumatic injuries; the 2 groups did not differ in overuse or serious injury rates. FMS & injury:-Short cycle group, candidates with a FMS score of < 14 had a 1.91 times (95% confidence interval = 1.21-3.01, P=<0.01) higher incidence of injury compared to those scored >14.-Long cycle group, candidates with a FMS score of < 14 were 1.65 times more likely to sustain an injury (95% confidence interval = 1.05-2.59, P=0.03) compared to those scored >14.-45.8% of persons with scores <14 suffered an injury compared to 30.6% of those with scores of >14. Physical fitness scores:-Relationship between FMS scores and physical fitness.-Physical fitness scores <280 were 2.2 times more likely to have FMS scores of <14 and significantly more likely to sustain an injury. |
75% |
| Teyhen et al. 2012 “The Functional Movement Screen: A Reliability Study” |
64 Army service members (53 males, 11 females) met the inclusionParticipants age range = 18 – 35 years old Novice examiners participating in this study consisted of 8 physical therapy students |
Cohort Study Four physical therapy students were randomly assigned to the participants to assess intra- rater test-retest reliability by assessing the FMS on day 1and day 2.Each rater measured between 14 and 18 participants.A second set of 4 physical therapy students were randomly assigned to view the participants’ movement simultaneously with the first set of raters for the inter- rater reliability assessment on day 2 |
FMS | FMS tested day 1 with 48 to 72 hrs between and day 2 retestTo minimise bias, raters were randomly assigned, raters for day 2 were kept blinded to day 1 raters’ measurements, pairs of raters on day 2 were blinded to each other’s analysis and scoring, and 48 to 72 hours of time elapsed between intra-rater test- retest reliability measurements. | The FMS has an adequate level of reliability when assessed in healthy service members by novice raters.The inter-rater agreement of the FMS component scores ranged from moderate to excellent, with 6 of the 7 tests categorized as having substantial agreement .The intra-rater and inter-rater point estimates of the FMS composite score reliability ranged from 0.74 to 0.76, with the 95% CIs suggestive of moderate to good reliability. | 78% |
Table 3: Summary and critical appraisal of included articles in this review.
Participants involved in the studies varied from male only19,28,29, to male and female participants26,27, from populations including firefighters19, Special Operation Soldiers26, Marine Officer Candidates28,29 and Army service members27. In all of the included articles the FMS was clearly defined and outlined. The use of the FMS throughout the studies varied slightly from confirming the reliability of the use of the FMS within the tactical population27 to use of the tool as a means of predicting injury potential28,29 and as a means of validating the effectiveness of training programs for tactical personnel19,26.
Only one study27 was found to investigate the reliability of employing the FMS tool within the tactical population. The study by Teyhen et al.27 was designed to determine the intra-rater and inter-rater reliability of the FMS when tested by a group of novice raters. In addition, the study also reported on the FMS component and composite scores of tactical population members27. Eight novice examiners, who were physical therapy students enrolled in their second and third semesters of a doctor of physical therapy training program, examined 64 Army service personnel with the FMS tool27. The examiners underwent 20 hours of FMS training conducted by four physical therapists and one research assistant. Four novice examiners were randomly assigned to the participants to assess intra-rater test-retest reliability by assessing the FMS on Day 1 and Day 227. The four novice examiners measured between 14 and 18 participants with no differences in outcomes across examiners27. To mimic field conditions that often include mass screening and multiple examiners, the remaining four novice examiners were randomly assigned to interpret the participants’ movement scores instantaneously with the first set of examiners on the second day of testing. To assess the intra-rater reliability, 48 to 72 hours of time elapsed between measurements27. To minimise bias for the inter- rater reliability assessment, examiners were blinded to any previous and ongoing results.
The researchers27 considered the FMS to have a moderate to excellent inter-rater agreement of the seven component tests with an intra-class correlation coefficient (ICC) of 0.76 (95% CI: 0.63, 0.85). It was also ascertained that there were considerable intra-rater agreement scores at 48 to 72 hours, which resulted in an ICC of 0.74 (95% CI: 0.60, 0.83). Teyhen et al.27 concluded that the FMS had an adequate level of inter–rater reliability within a group of novice examiners when assessing healthy service members and the inter-rater agreement of the FMS component scores were in substantial agreement.
Two studies28,29 investigated the potential for the FMS to predict the risk of injury within tactical populations. The study by O’Conner et al.29 was the first known large-scale study to be conducted within an active-duty military cohort. In this study, the researchers examined the utility of FMS during medical in-processing of 874 Marine Officer Candidates aged between 18 and 30 years of age29. All members of the research team were certified in the FMS to maximise inter-rater reliability29. The participants also completed a physical fitness test within the first week of starting their officer candidate training course29. These fitness tests consisted of pull-ups to exhaustion, two-minutes of abdominal crunches, and a three-mile (4.8km) run for time. Officer candidate training was divided into two groups; the first group completed a six-week training program and the second group completed a ten-week training program. During officer candidate training, injury data was captured daily in order to allow comparison of injuries to FMS prediction scores29. Physicians of the research team determined injury data by examining records of medical encounters of the subjects from external medical care providers. An injury was defined as physical damage to the body secondary to physical training with members seeking medical care one or more times during the study period29. Following the Marine Officer’s training, it was observed that personnel with an FMS score of <14, were 1.91 times more likely to sustain an injury and personnel completing the ten-week-long cycle were 1.65 times more likely to sustain an injury when compared to personnel with scores higher than 1429.
In 2013, Lisman et al.28 expanded on the findings of O’Connor et al.29. Using the same data, Lisman et al.28 investigated the associations between injuries and individual components of the Marine Corps physical fitness test, self-reported exercise participation and previous injury history, and FMS scores. Lisman et al.28 observed that, when including the time to complete a three mile (4.8km) run with FMS scores, the injury predictive value increased with officer candidates who scored poorly in both tests (FMS scores <14 and running time > 20.5 minutes) being 4.2 times more likely to experience an injury during Marine Corps officer training28.
Rather than focusing on injury prediction, the two remaining studies19,26 that met the inclusion criteria for this review focused on the ability of a physical training program to change FMS scores within their tactical populations. Frost et al.19 noted no significant changes in the total FMS for any group post training, whereas Gross et al.26 noted an improvement of FMS scores post training.
Frost et al.19 considered the practical application of the FMS within a tactical population of 60 male firefighters. Their study design included three groups: one control group and two intervention groups. The FMS was implemented by a certified FMS instructor prior to and following a 12-week physical training intervention provided by strength and conditioning professionals19. The results obtained revealed that there were no significant differences between groups in total FMS score prior to the 12 weeks of training (p = 0.838) or following the intervention (p > 0.176) 19. While no significant differences were found between groups, the base- line scores of 17 out of 26 participants that received an initial FMS score of < 13 exhibited an increase in FMS scores post training. Conversely 14 of the 17 participants who received a lower total post training score had a baseline FMS score of >1319.
In a tactical population of Special Operations Forces (SOF) soldiers, Gross et al. 26 employed the FMS tool to validate the effectiveness of a functional physical training program designed to prepare SOF soldiers for return to duty through reducing the gap between rehabilitation and return to duty, by enhancing movement performance and preventing injuries26. The study was conducted with 90 participants who were about to be discharged from physical therapy following extensive rehabilitation and healthy individuals who had not had any physical therapy26. The composition of these two groups (following rehabilitation or healthy) was not provided. Four physical therapy staff members administered the testing of the FMS, and the fitness tests pre- and post-six weeks of a training program26. The fitness tests conducted included a T-test for agility, six metre hop for time, single leg hop for distance, vertical jump, skin-fold body fat measure, balance test and core strength (kip-ups)26. Following the functional training program, FMS scores improved an average of 2.5 points, with improvements noted across all segments of the fitness tests. Gross et al.26 concluded that functional training programs are beneficial for soldiers returning to duty based on these increases in FMS scores. The researchers26 concluded that the FMS provided an effective tool for screening the tactical population and for validating the effectiveness of physical training programs.
Some constraints and variances were identified in the five studies employing the FMS in a tactical population. These included the availability of the participants to complete the study26 and a potentially higher fitness level of tactical personnel when compared to the general population19,26.The use of the tactical population encounters some restrictions when it comes to the participant’s availability that may limit their participation and completion of studies. Gross et al. 26 stated that within their study a number of participants were unable to participate in the follow-up due to a variety of reasons such as job requirements, time of day the research was conducted, and a lack of interest. Of the 155 participants that attempted the program, 65 (42%) participants dropped out of the training or were lost to follow-up26. Of the remaining 90 participants the mean number of intervention classes attended was 10 out of a possible 18 (56%)26.
The fitness level of the tactical population may also need to be considered when comparing the data to current research findings of non-tactical populations. O’Connor et al.29 and Lisman et al.28 stated that their sample of participants, who had been previously challenged and screened in the Marine Corps, were highly fit in terms of muscular strength, muscular endurance and metabolic (anaerobic and aerobic) fitness. With metabolic fitness in particular associated with injury risk in tactical populations, the high fitness of personnel within these populations may influence the ability of the FMS to predict injury in a tactical population31-33.
DISCUSSION
The aim of this review was to critically explore the literature on the potential use of the FMS tool within tactical populations given previous findings of its use in athletic21,23 and general populations10,22. Unfortunately, while the research reviewed was of good quality, the use of the FMS within tactical populations was found to be limited. Considering this, five articles19,26-29 were identified to examine the use of the FMS within tactical populations, with the focus of these articles being on reliability27, use as an injury prediction tool28,29 and use as a tool to validate tactical conditioning programs19,26.
For a tool to be used effectively in any population, it must be reliable. On this basis, Teyhen et al.27 investigated the reliability of the FMS within the tactical population. The results of their study suggested that raters (n=8) could, with moderate to excellent agreement, reliably employ the FMS tool in a tactical population (n=64 military personnel). Furthermore, their study results were comparable to the previous studies of Minick et al.34 and Onate et al.35. Minick et al.34 considered their raters (n=4) to have ‘excellent’ to ‘substantial’ agreement when assessing the FMS scores of 40 male and female college students. Similarly, Onate et al.35 considered their raters (n=2) to have a ‘high’ reliability in a similar University population of 17 male and female volunteers. On this basis, the FMS has the potential to be employed reliably within a tactical population.
O’Connor et al.29 and Lisman et al.28 both investigated the use of the FMS as an injury predictor within the tactical population through a large sample size of 874 participants. O’Connor et al.29 considered a score of <14 to be a viable score to predict injury. Lisman et al.28 expanded on this result to increase the predictive potential by including run times of > 20.5 minutes for a three mile (4.8 km) run. The result of these two studies, in regard to FMS scores, are consistent with current findings in other populations10,21-23. For example, Chorba et al.23 found that female collegiate athletes (soccer, volleyball and basketball players) that obtained an FMS score of <14 had a four-fold increased risk of lower extremity injury when participating in autumn l and winter sports. Likewise, Kiesel et al.21, found the FMS to positively predict injury in male National Football League players who scored below 14. It should however be noted that not all studies have found a relationship between FMS scores of below 14 and injury36,37. In studies investigating the injury predictive ability of the FMS on recreational runners36 and Basketball players37, no relationship between scores of below 14 and risk of injury were identified. Several potential reasons for these discrepancies in findings include; the variability between studies in regard to the definition of injury, previous injuries [e.g. history of ACL injury23] and differences in sporting populations and average FMS scores in these populations. As such, while there is some evidence supporting the potential of a score of <14 to predict injury, further research is needed. Considering this, the research of O’Connor et al.29 did note that, while not as pronounced as scores <14, participants who scored >18 on the FMS had a higher risk of injury than those scoring between 15-17 points. These results suggest a potential bimodal distribution of injury risk in relation to FMS scores.
While two papers19,26 investigating the use of the FMS to validate tactical conditioning programs were identified, no similar uses of the FMS in an athletic population could be found. One paper by Kiesel et al.20 however, considered how a conditioning program could be used to specifically improve FMS scores. The study found that a 7-week off-season intervention program could improve FMS scores (three points, p<0.01) and reduce the number of asymmetries in the group (from 50% to 34%, p=0.01). Chapman et al.38 conducted a similar study of 121 elite track and field athletes with corrective exercises prescribed following FMS screening. In addition, FMS scores were then compared to best performance results over two calendar years. While compliance with the corrective exercises were considered problematic and no results were provided, athletes with FMS scores of 14 or less did not improve in performance to the same extent that athletes with a score of higher than 14 (-2.3% versus 2.5% respectively). Similarly, subjects with an asymmetry had lower performance improvements than subjects with no asymmetry (2.10% versus 2.86%). These results suggest that for athletes with low initial FMS scores or an identified asymmetry, performance ability may be reduced.
As a final consideration, the study by O’Connor et al.29 considered the practical application of the FMS within the tactical population by adding the FMS to the medical screening of a large tactical cohort of over 800 personnel. While the intent of their study was to determine whether FMS scores could predict injury in a large military cohort29, the study also concluded that the FMS can be used as part of medical processing within the tactical population. While this application may be superfluous in non-tactical populations, the ability of the tool to be applied in a large, often time-poor, population may be valuable for tactical populations.
CONCLUSION
Occupational injury risk is prevalent within tactical populations such as police officers, firefighters and military personnel, who are required to carry external loads while performing daily duties. These external loads can affect their movement patterns and in turn lead to injury. Previous research in athletic and general populations suggests that the FMS is a reliable tool that may be of value in predicting injuries and even athletic performance. Results of this review suggest that the FMS tool may also be of use in tactical populations, employed as a reliable screening tool for either predicting the potential for injury or to determine the effectiveness of conditioning programs. Further research, specifically within tactical populations, is required to confirm and advance the findings presented in this review.