
ABSTRACT
Background
Long-term health conditions (LTHC) are major contributors to morbidity and mortality in Australia and may be more prevalent in Australian Defence Force (ADF) veterans. Previous analyses are limited because they do not control for age and sex confounding or disaggregate by ADF service status.
Purpose
We aimed to estimate and compare the age-standardised prevalence of self-reported LTHC by service status (current, former and never-serving persons). We also investigated associations between service status, sex, age and reporting of at least one LTHC.
Material and methods
We used 2021 Census data from the Australian Bureau of Statistics (ABS) to determine the prevalence of reporting LTHC by service status. Prevalence estimates were age-standardised using the ABS standard population. We estimated prevalence rate ratios (PRR) using Poisson regression.
Results
Crude prevalence was lower in current-serving persons and higher in former-serving persons compared with never-serving persons. After age-standardisation, these differences were attenuated, but remained: prevalence was lower in current-serving (2061 per 10 000) and higher in former-serving (3159 per 10 000) than in never-serving persons (2623 per 10 000). Older age and female sex were associated with a higher prevalence of reporting LTHC.
Conclusions
Reporting of LTHC was more prevalent among former-serving persons and less prevalent among current-serving persons than among never-serving persons. Age partly explained these differences, highlighting the importance of age-standardisation when comparing veteran and non-serving populations. The drivers of these differences are likely multifactorial and require further study.
Keywords:
Long-term health conditions, Australian Defence Force, Census data
Introduction
Noncommunicable diseases, such as ischaemic heart disease and cancer, were the leading cause of mortality among Australians between 1990 and 2019.1 These conditions also represent a substantial burden of morbidity: over half of the population in 2022 reported having a long-term health condition (LTHC), such as arthritis, asthma, back problems, cancer, and mental and behavioural conditions (including mood disorders, alcohol and drug problems and dementia).2 The prevalence of these conditions may vary across population groups.
Among Australian veterans, service experience has been associated with a higher prevalence of LTHC later in life.3 The Australian Institute of Health and Welfare (AIHW) used data from the 2020–21 National Health Survey and the 2020–21 National Study of Mental Health and Wellbeing to show that veterans (current- and former-serving persons) reported more LTHC than never-serving persons.4 This finding may reflect effects of wartime experience, age-related illnesses or policy changes relating to the assessment of war-related disability in the 1980s and 1990s in Australia.5 However, it is difficult to rule out any of these possibilities because of the small veteran sample size.
To overcome this issue, data from the 2021 Australian National Census of Population and Housing can be explored. The 2021 Census allows for population-level analyses of veterans because the ABS asked two new questions about people’s service with the Australian Defence Force (ADF)6 and their self-reported presence of long-term health conditions.7 Using this data, the ABS indicated a higher prevalence of reporting LTHC among former-serving persons compared to those who never served within most age groups.6 In contrast, current-serving persons report a lower prevalence of LTHC than those who had previously or never served; however, these comparisons were not presented by age group. These findings may reflect the general physical and mental fitness and younger age profile of the current-serving population.
While broadly informative, both the AIHW and ABS reports had important caveats. The AIHW report did not distinguish between service status (current, former, or never serving), despite these groups differing significantly in both age distribution and healthcare experience. Nor did it apply age-adjustment methods, such as standardisation, when comparing LTHC prevalence among veterans to that of persons who have never served. These constraints could not be addressed using the AIHW data due to the relatively small veteran sample. Similarly, although the ABS used a large, representative dataset from the 2021 Census, published comparisons of LTHC prevalence by service status were not age-standardised. While some results were disaggregated by age group, overall comparisons between service groups were not adjusted for differences in age distribution. This is important because the prevalence of reporting LTHC increases with age, and age distributions differ between current- and former-serving populations. As a result, crude comparisons may be confounded by age. Although age-group breakdowns provide useful context, they do not fully account for differences in age structure, making it difficult to determine whether observed differences reflect age or service-related factors. This may lead to misinterpretation of group-specific health burdens.
The primary aim of this analysis was to use 2021 Census data to compare the age-standardised prevalence of self-reported LTHC among current-, former- and never-serving persons. We also used regression to examine associations between service status and the prevalence of reporting at least one LTHC, and whether this differed by sex and age group. Individual LTHC were not analysed because the Census used self-reported data and short-form question types that are not diagnostic. Our findings provide population-level estimates of LTHC prevalence in these populations, which could be monitored over time to inform healthcare delivery, policy and practice, as well as future research directions.
Methods and materials
The ABS TableBuilder online tool was used to extract data (https://www.abs.gov.au/websitedbs/censushome.nsf/home/tablebuilder) from the 2021 Census of Population and Housing (Counting Persons 15 years or over). We extracted aggregate data by age group (15–64 years in 5-year bins), sex (male, female), ADF personnel service status (current-, former- and never-serving) and count of selected long-term health conditions7 (0, 1, 2, 3+). The data for veterans included regular and reservist members.6 We acknowledge that these cohorts are likely very different due to the nature of their work and workplace, and, where the numbers allow, in future studies, they should be separated. The age limit was necessary because there was no self-reported LTHC data for current-serving members aged 65 years and older. After all, compulsory retirement is 60 and 65 for regular and reservist members, respectively. Table 1 shows the estimated population distribution of current-, former- and never-serving persons used in the analysis. Estimates are presented because Census count values are slightly perturbed to protect the confidentiality of individuals. At the same time, these adjustments introduce small random errors; the ABS states that the overall information value of the data is not affected.8
Table 1
Population distribution by sex and service for persons aged 15–64 years answering the service question as extracted from ABS TableBuilder, 2021 Census, counting persons 15 years or over.
| Male | Female | |||||||||||
| Age (Years) |
Current serving |
% |
Former serving |
% |
Never serving |
% |
Current serving |
% |
Former serving |
% |
Never serving |
% |
| 15–19 | 2 448 | 4% | 502 | 0.3% | 674 834 | 10% | 858 | 5% | 197 | 0.5% | 642 747 | 9% |
| 20–24 | 10 131 | 16% | 2 845 | 2% | 712 566 | 10% | 3 347 | 20% | 1 002 | 2% | 702 443 | 9% |
| 25–29 | 11 007 | 17% | 7 736 | 4% | 775 569 | 11% | 3 179 | 19% | 1 670 | 4% | 804 941 | 11% |
| 30–34 | 10 159 | 16% | 13 679 | 8% | 791 083 | 11% | 2 602 | 15% | 2 533 | 6% | 868 928 | 12% |
| 35–39 | 8 642 | 13% | 15 782 | 9% | 791 949 | 11% | 2 070 | 12% | 3 008 | 7% | 859 112 | 11% |
| 40–44 | 6 128 | 9% | 17 430 | 10% | 713 093 | 10% | 1 486 | 9% | 4 369 | 10% | 764 735 | 10% |
| 45–49 | 5 448 | 8% | 23 636 | 13% | 696 456 | 10% | 1 297 | 8% | 5 660 | 13% | 762 128 | 10% |
| 50–54 | 5 170 | 8% | 30 858 | 17% | 676 046 | 10% | 1 144 | 7% | 8 195 | 19% | 751 059 | 10% |
| 55–59 | 3 917 | 6% | 35 020 | 19% | 646 393 | 9% | 657 | 4% | 7 946 | 19% | 719 177 | 10% |
| 60–64 | 2 473 | 4% | 35 797 | 20% | 613 408 | 9% | 381 | 2% | 8 090 | 19% | 693 418 | 9% |
| Total | 65 523 | 183 285 | 7 091 397 | 17 021 | 42 670 | 7 568 688 | ||||||
To calculate prevalence rates (PR, 95%CI) of self-reporting ≥1 LTHC in current-, former- and never-serving populations, we calculated crude rates and applied direct age standardisation using the ABS 2001 standard population, as recommended by the AIHW.9 We also undertook regression modelling to assess the influence of sex, age and service status on the prevalence of reporting at least one LTHC (yes/no). Poisson regression with a loglink function was used to estimate adjusted prevalence rate ratios (PRR, 95%CI) by age, sex and service status. PRRs were obtained by exponentiating model coefficients. The model was selected based on fit, as assessed by Akaike’s information criterion (AIC) and likelihood ratio tests. All analyses were performed using R software (version 4.2.3). The ‘epitools’ package (https://CRAN.R-project.org/package=epitools) was used for direct age standardisation, and the ‘MASS’ package (https://CRAN.R-project.org/package=MASS) was used for the negative binomial regression.
Results
Compared with never-serving persons, the crude prevalence of reporting ≥1 LTHC were 49% higher among former-serving persons and 32% lower among current-serving persons. After applying direct age standardisation, the prevalence of reporting ≥1 LTHC remained higher among former-serving persons (21%) than among current-serving persons (20%) compared with never-serving persons.
Table 2Crude and age-standardised prevalence rates (PR) for reporting long-term health conditions for current-serving, former-serving and never-serving persons.
| Service | Crude PR per 10 000 population (95% CI) | % change in PR with age standardisation | Age-standardised PR per 10 000 population (95% CI) |
| Current serving | 1 837 (1 811–1 864) | 12% | 2 061 (2 031–2 099) |
| Former serving | 4 032 (4 012–4 053) | -22% | 3 159 (3 123–3 195) |
| Never serving | 2 705 (2 702–2 707) | -3% | 2 623 (2 621–2 626) |
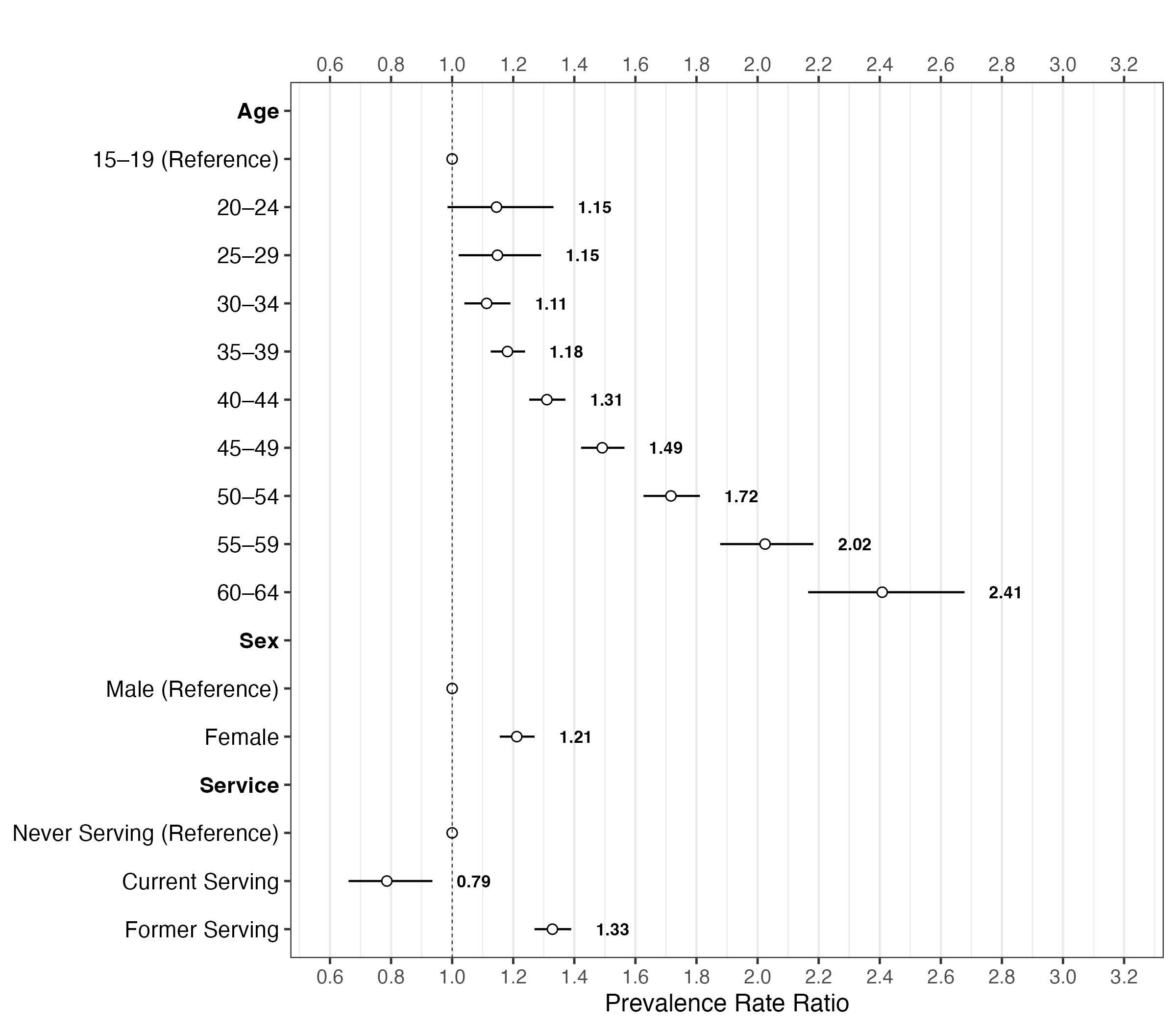
Controlling for age and service in the regression, we found that females had a higher prevalence of reporting LTHC than males (PRR 1.21, 95%CI 1.16–1.27). When sex and service were controlled, we found that older age was strongly associated with LTHC, such that 60–64 year olds had a higher prevalence of reporting LTHC (PRR 2.41, 95%CI 2.17–2.68) than 15–19 year olds (see Figure 1). It is important to note that while the Census reports data for the 15–19-year age group, the ADF’s age requirement for entry is 17; therefore, this likely captures only ADF members aged 17–19. When controlling for age and sex, the differences between services remained. Compared with never-serving persons, current-serving persons had a lower prevalence of reporting LTHC (PRR 0.79, 95%CI 0.66–0.94), whereas former-serving persons had a higher prevalence (PRR 1.33, 95%CI 1.27–1.39).
Discussion
Our study sought to address considerations raised in previous analyses by applying direct age standardisation and distinguishing between current- and former-serving ADF persons. We observed three key findings. First, compared with those who have never served, the crude PR of self-reporting a LTHC was lower among current-serving persons and higher among former-serving persons. Second, the observed differences persisted after age standardisation, but their magnitude decreased across all comparisons, underscoring the importance of controlling for age when comparing veteran to never-serving populations. Third, being older, female and former-serving was associated with a higher rate of reporting LTHC.
Several factors may help explain the lower prevalence of LTHC among current- versus never-serving persons. These include: 1) selection bias during enlistment, whereby recruitment standards select for healthy persons; 2) protective factors when in service, whereby full-time members maintain a high level of health and regularly access funded healthcare services through Defence; or 3) potential underreporting due to lower levels of healthcare seeking or fear of career implications. In contrast, the prevalence of LTHC in former-serving versus never-serving persons may reflect both service-related and non-service-related health conditions. Some former service members may have left the service due to health issues. In contrast, others may be more aware of, or more likely to report, health conditions due to regular or continued contact with the healthcare system during or after service.
It is challenging to determine the extent to which these conditions are directly attributable to exposure during service, given the multifactorial nature of many chronic illnesses. Nonetheless, evidence suggests the ADF has a higher incidence of serious medical claims compared to the general population, and in 2015, 61% of former-serving persons accessed care through the Department of Veterans’ Affairs for service-related conditions.10 The prevalence of self-reporting LTHC in the context of accessing insurance or benefit-driven healthcare is important because there exists an association between undergoing a claims process and poorer health outcomes10. While previous research has indicated that exposure to conflict is a likely factor in future LTHC for Vietnam veterans,3 our analysis only included persons aged between 15 and 64 years, thereby likely excluding most, if not all, members who would have served in Vietnam.
Our findings are based on the Census, which provides near-complete population coverage, with a non-response rate of only 6% to the service question (https://www.abs.gov.au/census/find-census-data/quickstats/2021/AUS). While this enhances generalisability, several limitations should be acknowledged. First, health conditions were self-reported; these findings are only estimates of LTHC prevalence. Further research is warranted to confirm these findings and identify the driving factors of the observed differences. Second, the Census question on ADF service did not distinguish between service branches (Army, Navy, Air Force), precluding any analysis of variation in health outcomes by branch. Future research should allow for disaggregating by service branches.
Despite these limitations, our findings reinforce the importance of distinguishing between, and controlling for the age of, current- and former-serving populations when assessing veterans’ health. These groups differ significantly in age, service experience and access to health services. Future research that does not account for service status or control for age risks may draw misleading conclusions about the health burden faced by ADF personnel. We recommend that future studies further disaggregate veteran populations—by branch, service length and exposure—and explore causal pathways using longitudinal or linked administrative data.
Please specify the URL of your file