
Abstract
Evidence suggests that standard triage models are not adequate in threat-moderated settings like terrorist or intentional mass-violence events. Ten Second Triage offers an alternative triage model based on traumatic wounding patterns and immediate interventions for preventable causes of death, rather than physiological parameters. Over-triage may occur due to first responders’ low tolerance for tourniquet application during Ten Second Triage. There is an opportunity to deconflict over-triage post-rescue before transport to lessen surge burden and clinical complexity for first receivers, utilising the tourniquet traffic light as a deconfliction tool.
Discussion
The utility of standard triage models within the operational milieu of an intentional mass-violence incident and terrorism is often called into question.1 Triage models, such as Simple Triage and Rapid Treatment (START) and Sort-Assess-Lifesaving Interventions-Treatment and/or Transport (SALT), rely on physiological parameters that can be cumbersome and time-consuming to apply. Historically, the application of these triage models has often been poor or skipped in favour of rapid rescue and evacuation.2 While this leads to the prehospital area of operation being cleared quickly, the congestion from poorly or untriaged patients shifts to the secondary care facility, creating a bottleneck and draining resources. Ultimately, patients will need triage, whether first responders perform it or the responsibility is passed to the first receivers. Triage is essential to ensure that clinical resources are allocated efficiently for the greater good.
To reduce triage complexity, Vasselo et al.3 developed the Ten Second Triage (TST) model. TST disregards physiological parameters in favour of wound patterns and interventions that address the immediately preventable causes of death as indicators of injury severity. The model is straightforward enough for a range of responders, including police, fire and ambulance personnel.3 Its application is quick, allowing for simultaneous action on preventable causes and subsequent triage. The model is highly beneficial for response systems that can exploit the inner zones (warm/hot) of care.3 However, due to the model’s rapid interventional speed and the low tolerance for bleeding among first responders in threat-moderated environments, there is a risk of over-triage when immediate action tourniquets (TQ) are applied. Notably, the TST categorises non-ambulatory casualties with a limb tourniquet in situ as being within the highest triage grouping (P1), thus assigning a clinically equivalent priority to casualties with either penetrating abdominothoracic trauma or airway obstruction (Figure 1).
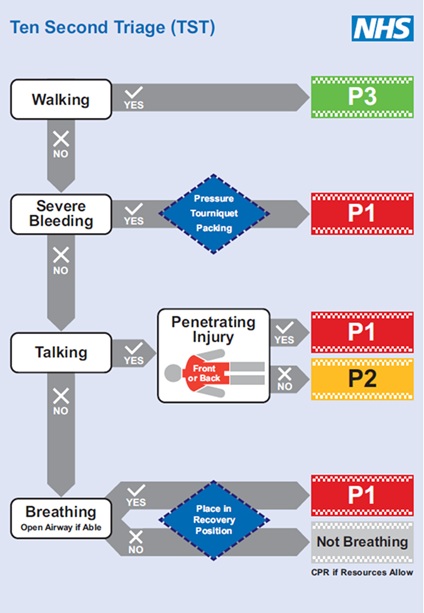
Figure 1. Ten Second Triage model. Vassallo, et al. (2024).3
Ambulatory casualties with limb tourniquets in situ are by default assumed to have severe bleeding, which escalates triage classification (P1).3
The Kerslake report, following the 2017 Manchester arena bombing, noted that bystanders attempted TQ application without sufficient training, implying that their efforts were at risk of being ineffective or misapplied.4 Hedger et al.5 assert that an increasing proportion (77%) of prehospital TQ applications are not medically indicated in civilian trauma care. Similar trends have likewise been described in the management of military penetrating limb trauma in combat casualties.6 Therefore, based on the evidence, it is reasonable to assume that in threat-moderated settings, TQ application is likely to be excessive to medical requirements, resulting in a larger proportion of over-triaged patients when TST is used.
An opportunity for over-triage deconfliction exists before allocation and transportation to secondary care facilities. Patients who may have been managed with TQ application during warm zone care by bystanders or first responders should be assessed for TQ conversion when resources become available. The authors propose that a system of early TQ evaluation and de-escalation be formalised at the Casualty Collection Point (CCP) to deconflict TQ-associated over-triage prior to transport in mass casualty events. One method of achieving this is the assignment of a Tourniquet Conversion Officer, who is positioned at the CCP Triage Point or is mobile within the CCP treatment area. Tourniquet conversion is a skill that is seldom the focus of prehospital haemorrhage control in the civilian setting, given the efficiency of mature prehospital systems.5 Evidence from the Russo-Ukrainian war shows that the nexus of low tolerance for tourniquet application, failure to convert tourniquets and prolonged evacuation exacerbated by battlefield conditions has contributed to a high burden of tourniquet-related complications.7 Intentional mass-violence incidents are low-frequency, high-consequence events resembling threat-moderated battlefield settings.8 Therefore, TQ conversion becomes a tactically essential skill to minimise harm and prevent issues not often found in non-threat-moderated conventional prehospital settings.
The strategic rationale for this process is to identify TQs applied under warm or hot zone conditions that are deemed medically unnecessary, enabling early TQ conversion and casualty reclassification according to the TST into a lower-priority group. Conversion involves controlled TQ release following wound packing, preferably with haemostatics and pressure bandaging.9 If TQ conversion is successful and no additional confounding injuries are noted, the patient can be re-categorised according to a more detailed assessment, as described by Vassallo et al.3
In the event of mass casualty events, the authors recommend using the TQ Traffic Light to aid triage reclassification (Figure 2).10 The TQ Traffic Light is a temporal model of tourniquet safety, segregated into 2-hour intervals from the time of injury to the restoration of blood flow to the injured limb. While the first 2 hours post-injury and TQ application are generally considered safe, the 2-hour interval is marked by changes in safety parameters as indicated by a set of observed physiological indicators. Pascoe and Weinrauch11 demonstrate, through a review of the evidence, that at the 2-hour mark, TQ safety is less assured, based on marked intramuscular acidosis, cellular necrosis and endothelial leakage, which leads to the early onset of ischaemic injury and reperfusion compartment syndromes.11 Similarly, Lukiianchuk et al.12 reviewed Ukrainian casualties, finding that after 7 hours of tourniquet use, all patients develop compartment syndrome, with 70% needing dialysis, 36% amputations, and about 7% experiencing related deaths.12 Thus, if the total forecast time after rescue, including initial TST triage, transport and secondary triage, exceeds 2 hours, TQ conversion should be attempted before transport to reduce harm and prevent complications.
A TQ conversion at this point serves two purposes: first, to deconflict triage and accurately direct the use of first-line care and evacuation resources; and second, to reduce the compounding of clinical complexity for first receivers at the destination facility. If TQ conversion at this point is successful, the patient can be re-categorised using more precise criteria, potentially reducing surge load, clinical resource allocation and complexity at receiving facilities.
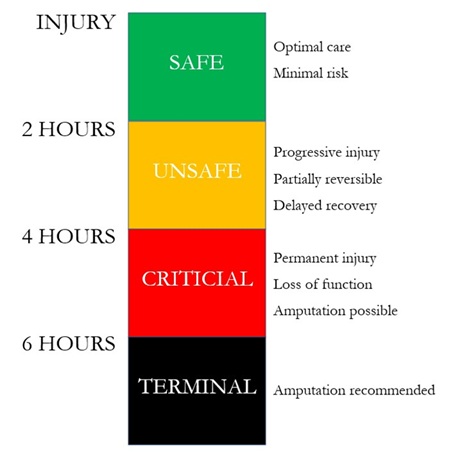
Figure 2. The Tourniquet Traffic Light. Weinrauch (2023).10
Conclusion
TST represents an evolution in mass-violence response, shifting focus from physiological determinants of severity to a simultaneous wound pattern and interventional triage model. While its rapid wound-pattern assessment significantly improves efficiency, the model’s risk of tourniquet-driven over-triage demands structured mitigation. The proposed two-phase deconfliction protocol, which involves tourniquet conversion at casualty collection points guided by the TQ Traffic Light framework, directly addresses this challenge. By reclassifying patients before transport, this approach achieves three vital outcomes:
- Reduces surge burden on receiving facilities
- Minimises clinical complexity for first receivers
- Preserves TST’s lifesaving speed while enhancing accuracy for more detailed assessment.
This integrated strategy transforms TST from a triage tool into a more comprehensive system that balances urgency with precision, ultimately optimising resource allocation across the continuum of care during intentional mass-violence events. Future validation should focus on operationalising the TQ Traffic Light framework in multiagency intentional mass-violence drills.
Please specify the URL of your file