
Abstract
Introduction US Army Reserve personnel are expected to meet the same fitness and readiness standards as their Active Duty counterparts, but little is known about health factors among Reservists. This investigation presents data on injuries, fitness and body mass index (BMI) for Reservists participating in a new health and fitness program.
Methods Twenty-one US Army Reserve units were selected to participate. Electronic surveys were administered in 2021 to collect baseline data on recent injuries, fitness and demographics. Demographics and injury details were summarised. Differences in injury prevalence by BMI and aerobic fitness (Army Combat Fitness Test (ACFT) 2-mile run time) were reported.
Results Among the 2095 baseline survey respondents, most were male (72%), white (60%) and 30 ± 10 years old on average. More than a quarter of men (28%) and over one-third of women (35%) reported at least one injury in the previous 12 months. Commonly reported injuries included strains (19%) and sprains (12%), often involving the lower back (21%) or knees (19%), and were frequently attributed to running (22%) or weightlifting (18%). Over half of respondents (57%) passed the ACFT. About one-quarter of men (24%) and 16% of women were classified as obese. Men and women classified as obese had an injury prevalence 1.6 times higher than those with normal BMI (p<0.001). Likewise, injury prevalence among women with slower 2-mile run times was 1.6 times higher than the fastest runners (p<0.05).
Conclusion Injuries in this sample of Reservists were similar to those reported in other military populations despite differing exposures and demographic distributions. Maintenance of a healthy weight status should be emphasised for Reservists, along with appropriate physical training resources for military duties. These results should inform future public health programming in the US Army Reserve.
Introduction
The United States (US) Army Reserve Command (USARC) is a unique population that is not often included in standardised US Army medical data surveillance. Nearly 170 000 US Army Reservists serve in units located across all 50 states and five territories.1 Most US Army Reservists serve part-time, one weekend per month and two weeks per year, often holding civilian occupations in addition to military service. However, Reserve personnel may be deployed to full-time Active Duty (AD) service.1 As a result, US Army policy requires Reservists to meet the same fitness and readiness standards as their AD counterparts, including successfully completing the Army Combat Fitness Test (ACFT). The ACFT consists of six events; each individual event must be passed to pass the test.2 Reservists are required to pass the ACFT annually in order to remain active and be eligible for promotion.3
Despite the importance of readiness for all military troops, most US military health surveillance and investigations are focused on AD personnel. Therefore, less is known about injuries, physical fitness and other health factors among US Army Reserve personnel.4 Medical encounter surveillance indicates that injuries are the leading reason for medical visits at Military Treatment Facilities among US Army Reserve personnel,5 though this does not capture injuries treated outside of the Military Health System. Previous studies of Reservists indicated that, on average, Reservists are older,6 have higher body mass index (BMI),6,7 spend less time performing physical training,8 and are less physically fit based on physical fitness test performance4, 8 when compared to AD personnel. Studies of Reserve members from the Australian and British Armies have suggested similar trends and also explored injury data,9-14 but comprehensive details about injuries and fitness among US Army Reservists have not been previously reported in the literature.
Injuries are consistently a leading reason for medical care among AD Army Soldiers, leading to over 2 million medical encounters and 8 million days of limited duty annually.15 A majority of injuries among AD Soldiers (~70%) are musculoskeletal overuse injuries,15 often resulting from physical training. Higher BMI and slower 2-mile run times (i.e., lower aerobic fitness) have been associated with increased injury risk in AD US Army populations.16-18 However, these relationships have not been extensively investigated for Reserve personnel. This article summarises relationships between injuries, physical fitness and obesity among a cohort of US Army Reservists.
Methods
This project was reviewed and approved as public health practice by the Public Health Review Board of the authors’ institution (PHRB #20-876). Informed consent was obtained from all respondents prior to participation. An electronic survey was administered from July–December 2021 to US Army Reserve units participating in the baseline portion of a new health and fitness program, and results were briefly described previously.19 USARC identified 21 participating units. Data collected included demographics, recent ACFT performance,20 and details about injuries in the previous 12 months. Survey data was used for all metrics for consistency, as self-report is the most feasible way to collect comprehensive injury data for this population since Reservists may not always utilise Military Treatment Facilities for medical care..
Injuries were defined as bodily tissue damage resulting from an external energy transfer, either occurring suddenly (acute) or gradually developing over time (overuse), in accordance with the standardised military surveillance injury definition.21 Respondents provided information for up to two of their most physically limiting injuries in the 12 months prior to survey administration, including injured body area, type of injury and activity causing the injury. The five most frequently reported injury types, injured body regions and injury activities are summarised.
SPSS© v.26 was used for all statistical analyses. BMI distribution and ACFT performance statistics are presented and stratified by sex. BMI categories were defined by the Centers for Disease Control and Prevention22 and Army Body Composition Regulations,23 using reported height and weight. ACFT pass/fail status was determined using 2021 scoring standards,24 and only respondents reporting complete data for all events were included in the analyses. ACFT 2-mile run performance was binned into equal quartiles for analysis. Injury prevalence is reported by BMI and ACFT 2-mile run performance for both sexes. Chi-square tests were used to analyse statistically significant differences in frequency data. Unless noted, averages are reported as mean ± standard deviation (SD). Statistically significant differences were identified by p<0.05.
Table 1. Demographics of Pilot Program Reservists
| Categories | n (%) |
|---|---|
| Sex | |
| Male | 1517 (72) |
| Female | 563 (27) |
| Prefer not to answer | 15 (1) |
| Race | |
| White | 1251 (60) |
| Black | 593 (28) |
| Other | 251 (12) |
| Age | |
| <25 | 706 (34) |
| 25-34 | 784 (37) |
| 35-44 | 384 (18) |
| ≥45 | 221 (11) |
| Rank | |
| Junior Enlisted (E1-E4) | 980 (47) |
| Senior Enlisted (E5-E9) | 632 (30) |
| Junior Officer (O1-O4) | 410 (20) |
| Senior Officer (O5-O6) | 47 (2) |
| Warrant Officer or Other | 26 (1) |
| Marital status | |
| Single, never married | 1047 (50) |
| Married | 806 (39) |
| Other/unknown | 242 (11) |
| Highest education level | |
| High school or less | 980 (47) |
| Associate’s degree | 358 (17) |
| Bachelor’s degree or higher | 708 (34) |
| Other/unknown | 49 (2) |
Table 2. Leading injury types, injured body parts and injury activities by sex (n=858 injuries among Pilot Program Reservists)
| Male respondents n=589 injuries n (%) |
Female respondents n=269 injuries n (%) | ||
|---|---|---|---|
| Injury type | |||
| Strained muscle | 120 (20) | Strained muscle | 43 (16) |
| Sprained joint | 80 (14) | Overuse muscle pain | 27 (10) |
| Pain | 66 (11) | Sprained joint | 25 (9) |
| Runner’s knee (pain on/around the kneecap) | 41 (7) | Pain | 25 (9) |
| Overuse muscle pain | 31 (5) | Fracture | 10 (4) |
| Injured body part | |||
| Lower back | 128 (22) | Knee | 54 (20) |
| Knee | 119 (20) | Lower back | 49 (18) |
| Shoulder | 67 (11) | Shoulder | 38 (14) |
| Ankle | 45 (8) | Ankle | 20 (7) |
| Foot | 32 (5) | Foot | 18 (7) |
| Injury activity | |||
| Running | 128 (22) | Running | 62 (23) |
| Weightlifting | 106 (18) | Weightlifting | 45 (17) |
| Lifting heavy objects | 65 (11) | Lifting heavy objects | 35 (13) |
| Sports | 31 (5) | Walking/hiking | 13 (5) |
| Walking/hiking | 19 (3) | Sports | 21 (8) |
Table 3. Army Combat Fitness Test (ACFT) performance by event and sex (n=1187 Pilot Program Reservists with complete ACFT data)
| ACFT event | Males | Females | ||||
|---|---|---|---|---|---|---|
| Participants (n) | Average performance | Pass (%) | Participants (n) | Average performance | Pass (%) | |
| Deadlift (pounds) | 914 | 202 ± 70 | 94 | 273 | 156 ± 38 | 91 |
| Power throw (metres) | 914 | 9.5 ± 2.5 | 99 | 273 | 6.1 ± 2.5 | 83 |
| Hand-release push-ups (repetitions) | 914 | 29 ± 14 | 99 | 273 | 19 ± 10 | 99 |
| Sprint-drag-carry (minutes) | 914 | 2:24 ± 1:26 | 91 | 273 | 2:46 ± 0:38 | 74 |
| Leg tuck (repetitions) Alternate: Plank* |
911 21 |
7 ± 6 – |
94 81 |
273 85 |
2 ± 4 – |
47 77 |
| 2-mile run Alternate: bike or row† |
881 33 |
17:47 ± 2:53 – |
92 55 |
268 6 |
20:07 ± 3:11 – |
71 50 |
| Overall¥ | 914 | – | 78 | 273 | – | 48 |
*In this version of ACFT, those who failed the leg tuck event could participate in an alternate plank event.
†ACFT participants on profile for the 2-mile run event could participate in an alternate aerobic event.
¥Passing all events was required to pass the ACFT overall.
Figure 1. Distribution of BMI by Sex (n=2,080 Reservists; Males n=1,517, Females n=563)
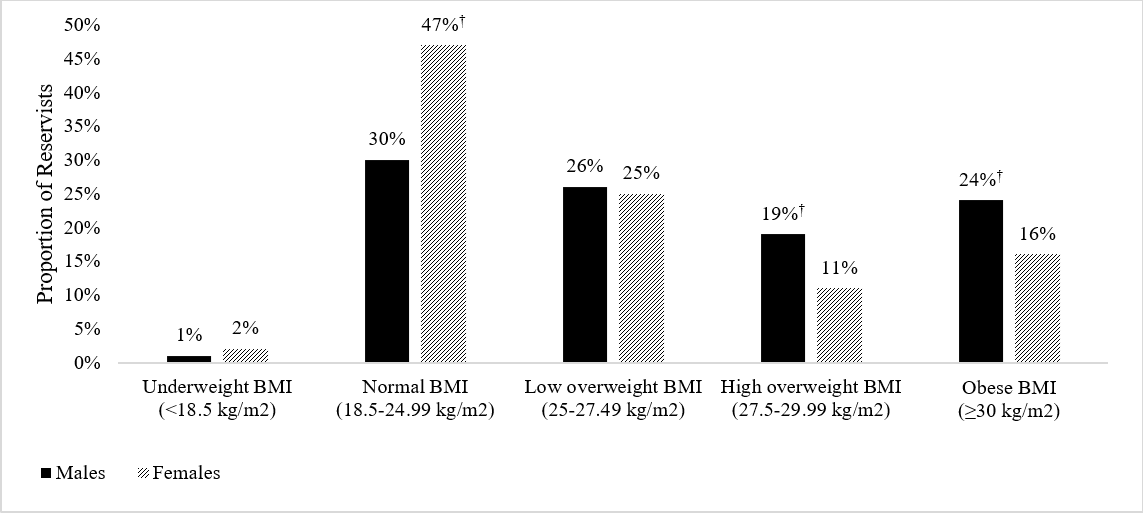
†Indicates that the proportion of Reservists in the BMI category is higher compared to the proportion for the other sex (p<0.001).
Figure 2. Percent Injured by BMI (n=2,080 Reservists; Males n=1,517, Females n=563)
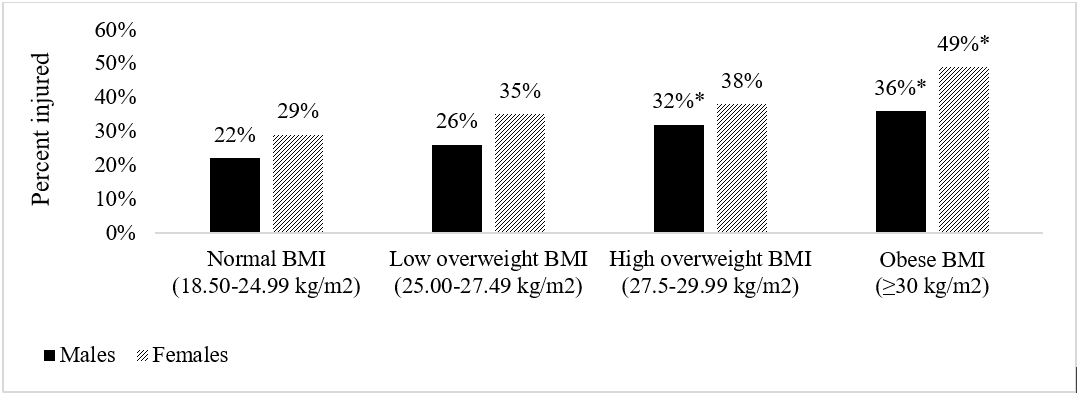
*Indicates that the proportion of Reservists reporting at least one injury is higher than the proportion injured among those who reported normal BMI (p<0.05).
Normal BMI: n=477 males, n=263 females
Low overweight BMI: n=400 males, n=153 females
High overweight BMI: n=289 males, n=61 females
Obese BMI: n=366 males, 92 females
Figure 3. Percent Injured by ACFT 2-mile Run Performance, with BMI distribution
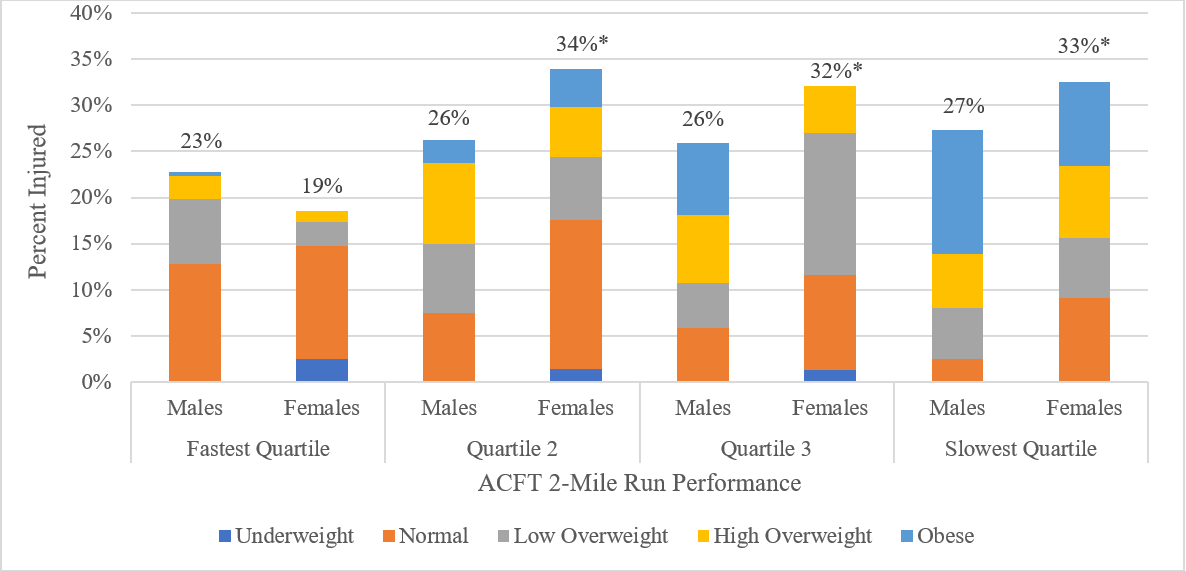
*Indicates that the proportion of Reservists reporting at least one injury is higher than the proportion injured among those with the fastest ACFT 2-mile run performance (p<0.05).
Fastest quartile: n=242 males ≤15.8 minutes, n=81 females ≤18.5 minutes
Quartile 2: n=239 males 15.9-17.7 minutes, n=74 females 18.6-20 minutes
Quartile 3: n=243 males 17.8-19.5 minutes, n=78 females 20.1-21.6 minutes
Slowest quartile: n=238 males >19.5 minutes, n=77 females >21.6 minutes
Results
There were 2095 survey respondents who provided sufficient responses for sex, height, weight and recent injuries. Most survey respondents were men, white, enlisted, and single (Table 1). The average age was 30 ±10 years old. A diverse distribution of military occupational specialties was represented, with the most common specialties being military police (21%), medical (21%) and engineering (19%).
Over one-quarter of respondents (30%, n=626) reported experiencing at least one injury in the previous 12 months. Respondents provided information for a total of 858 injuries (589 among male respondents (69%), 269 among female respondents (31%)). The five most frequently reported injured body regions, injury types and injury activities are summarised in Table 2 by sex. The leading reported injury type for both sexes was strained muscle, followed by sprained joints for men and overuse muscle pain for women. The most frequently injured body parts for both sexes were the lower back and shoulders. Activities frequently associated with injuries included running, weightlifting and lifting heavy objects. Overall injury prevalence was 28% and 35% for males and females reporting at least one injury, respectively.
Table 3 shows event performance and pass rates for respondents’ most recent ACFT. Over half of respondents (52%, n=1094) reported participating in an ACFT and provided complete data for all six events. Compared to female respondents, male respondents had higher pass rates for all events (p=<0.001-0.06), except hand-release push-ups for which both sexes had the same pass rate. The sprint-drag-carry, 2-mile run and leg tuck/plank events had the lowest pass rates for both sexes. More male respondents reported performance consistent with overall passing scores than female respondents (p<0.001).
The average BMI was 27 ± 4 kg/m2 among male respondents and 26 ± 4 kg/m2 among female respondents. BMI distributions for both sexes are shown in Figure 1. A higher proportion of female respondents were in the normal BMI range compared to male respondents (p<0.001, Figure 1). In contrast, higher proportions of male respondents had BMIs classified as overweight and obese compared to female respondents (p<0.001, Figure 1).
When considering the impacts of BMI on injuries in this population, both male and female respondents with higher BMIs had higher injury prevalence (Figure 2). On average, male respondents with BMIs classified as high overweight or obese had a higher injury prevalence compared to male respondents with normal BMI (p=0.006 and p<0.001, respectively). Similarly, female respondents with BMIs classified as obese reported a higher injury prevalence compared to female respondents with normal BMI (p<0.001).
Sixty-one percent of respondents (n=1272) reported completing an ACFT 2-mile run event in the previous 12 months. Female respondents who reported the fastest 25% (quartile (Q)) run times had a lower proportion of reporting injuries compared to slower female runners (Q1 vs Q2 p=0.30, Q1 vs Q3 p=0.049, Q1 vs Q4 p=0.04; Figure 3). A similar trend was noted for male respondents, but differences were not statistically significant (Q1 vs Q2 p=0.36, Q1 vs Q3 p=0.41, Q1 vs Q4 p=0.25). For both sexes, a significantly higher proportion of injured Reservists in the slowest run quartile were obese (p<0.05) compared to other run quartiles.
Discussion
This study is one of the first to report demographic, injury, fitness and BMI data among US Army Reserve personnel, a unique and understudied military population. Population demographics indicated a higher proportion of females and an older average age than in AD Army.15 Demographics in this subpopulation were similar to those reported in a 2022 USARC report summarising the full Reserve population.25
The most frequently reported injured body regions and injury types in this Reserve population were similar to those typically observed among full-time AD Service Members.26 Reservists predominantly reported injury types consistent with cumulative musculoskeletal overuse injuries, which is also the most common category of injuries among AD personnel.15,26 Activities associated with Reservists’ injuries were primarily related to physical training and occupational exposures, which are similar to injury activities often reported in AD military populations.16,26 The 30% injury prevalence in this population, however, was lower than what has been observed in analyses of Army AD medical records,15 and lower than self-reported injury prevalence in many previous studies of AD populations.27,28 This may be expected because Reservists, given their part-time status, may perform less physical training and could therefore experience fewer training-related injuries.4,8 Studies of AD and Reserve populations in other countries have also observed similarly lower injury rates for Reservists compared to AD.10,11 Women had a higher prevalence of injuries in this population (35% injured) compared to men (28%), which reflects a similar trend observed among US Army AD Soldiers,15 and also in another study among Reservists.4
Reserve personnel in this population reported lower ACFT event performance than has previously been reported for AD Army Soldiers.15 Previous studies have also shown that Reservists experience more fitness test failures compared to AD.4,8 These differences suggest that the Reserve health and fitness program should focus on improving physical fitness.
About one-quarter (24%) of males and 16% of female Reservists in this population reported height and weight consistent with a BMI classified as obese, which is higher than the reported obesity prevalence for AD service members15 but lower than the obesity rate among US adults.29 Another previous study similarly observed that a sample of US National Guard and Reserve members had higher obesity rates than AD military.30 A BMI classified as obese has been associated with lower performance on the US Army Physical Fitness Test.31
The associations between injuries, physical fitness and BMI have seldom been explored for US Army Reserve members. This analysis showed that the prevalence of injuries for both sexes was higher with higher BMI or slower 2-mile run performance, which is consistent with relationships previously observed among AD Army Service Members.17
Reservists are expected to meet the same fitness standards as AD Service Members2 but with much less oversight of physical training. Therefore, it has been suggested that additional fitness programs may be needed to encourage more effective physical training among Reservists.9,32 One proposed suggestion for Reservists is a mixed training approach with three 50-60-minute weekly exercise sessions that combine aerobic, anaerobic, muscle strengthening and occupation-specific tasks.32 Another recommendation is to encourage small group training with other Reserve personnel when possible, to build a similar community training focus as AD personnel.9,32 Regulation and enforcement from leadership would be necessary if specific training activities were required.
Increasing physical training among Reservists may be challenging because exercise is primarily conducted during personal time and using personal resources. Despite this, a previous study found that Reservists reported existing levels of physical training that, on average, exceed national exercise recommendations.7 However, another study observed that AD Service Members participated in more high-intensity interval, resistance and vigorous physical training than Reservists.8 Therefore, to improve strength and power, Reserve personnel should perform physical training that includes vigorous cardiorespiratory activities (e.g., running, sprints, high-intensity interval training, etc.) and at least two days a week of muscle-strengthening exercises. Ensuring access to physical fitness instructors can help Reservists train specifically for US Army duties. These physical training adjustments may enable Reservists train in a similar manner to their AD counterparts. However, mental and physical demands resulting from civilian occupations should also be considered when planning individual fitness programs for Reservists, in addition to their military service and training requirements.
Strengths and limitations
This is one of the first known investigations of demographics, physical fitness, injuries and BMI among US Army Reserve members. However, there are some limitations to note. The study population was a subset of Reservists from the Southeast region of the US; data may not represent all Reservists, and future work should analyse outcomes in a broader sample of Reservists if possible. Also, the calculated BMI outcome cannot differentiate between lean body mass and fat mass; however, previous studies have found BMI to have moderate to strong correlations with body fat percentage (0.65–0.95), including among military personnel.33,34 Finally, although self-reported survey data may be subject to recall bias, previous analyses have shown that military survey respondents accurately report their injury, height, weight and fitness test performance information.35,36 However, a previous study found that when military members were asked to recall past injuries, recall decreased as time passed,35 so injuries reported in this population may have been underestimated.
Conclusion
This work provides important information about health factors in an understudied military population. US Army Reservists reported similar injuries as those often experienced by their AD counterparts, predominantly overuse lower extremity injuries resulting from physical training. About one-quarter of males (24%) and 16% of females reported having a BMI classified as obese, and a significantly greater proportion of those with higher BMIs reported at least one injury. Female respondents with the fastest ACFT 2-mile run times had the lowest proportion of reporting at least one injury compared to slower female respondents. Given these observed relationships between injuries, BMI and aerobic fitness, health and fitness programs for US Army Reservists should emphasise maintenance of healthy weight status and appropriate physical training for US Army duties.
Corresponding Author: Anna Schuh-Renner, anna.s.renner.civ@health.mil
Authors: A Schuh-Renner1, T Grier1, O Mahlmann1, R Waring2, M Canham-Chervak1
Author Affiliations:
1 Defense Health Agency Public Health
2 US Army Reserve Command