
Introduction
The military-to-civilian transition (MCT) is a significant life change for military personnel. Characterised as the process of leaving the military and returning to family, community and workplace roles,1 a successful transition is widely considered essential for supporting veterans’ wellbeing in civilian life.2 Globally, over 200 000 military personnel transition to civilian life each year.3 While most veterans transition successfully, a substantial proportion experience reintegration challenges.4-6 Transition challenges include increased risk of mental health disorders such as depression and anxiety disorders, social isolation, difficulties securing employment, strained family relationships and financial hardship.4,7,8 In addition to the social costs, adverse transition outcomes also represent a sizeable financial burden, with the annual costs associated with adverse transition outcomes in the United Kingdom (UK) alone estimated at £258 million.9 Ensuring a successful transition for veterans on completion of their military service, therefore, has the potential to significantly reduce both financial and social burdens to individuals and the broader community. Emerging evidence suggests that multiple factors, including psychological health, physical wellbeing, economic stability and social relationships, shape MCT outcomes.10-12 Among these, social factors have received growing attention for their potential to facilitate successful reintegration.12 Within the social domain, several constructs have been implicated in supporting veterans during transition. These include social connectedness,13 social identity,14 and broader forms of social support that foster belonging and integration into civilian networks.13 The presence of loneliness—potentially the opposite of social connection—has been associated with negative transition experiences.15 Higher levels of all these social resources are associated with fewer symptoms of depression, anxiety, post-traumatic stress disorder (PTSD) and general psychological distress in veterans.16,17 This growing evidence suggests that social support factors may act as protective transition mechanisms.
Research on social support in the context of MCT is methodologically diverse, with variations in conceptual frameworks, measurement tools and recruitment strategies. Variety in methodology increases the scope during the conceptual phase of a construct. However, as social support factors have now been established as playing a role in transition, this lack of consistency limits the synthesis of findings and the ability for interventions to build on the strengths of earlier work. For example, qualitative research designs exploring how veterans’ social experiences influenced their transition to civilian life,18 or their social reintegration difficulties,19,20 do not appear to use the same psychological constructs as many cross-sectional designs exploring associations within the same topic.21,22 This diversity in approach is further reflected in the measurement tools and theoretical frameworks used to understand the MCT. This includes life-course, sociological and wellbeing-oriented frameworks.2,10,11
It is also unclear how well veteran recruitment strategies allow studies to extrapolate to the broader veteran population. In fact, in many countries, the ability to determine the proportionality of veteran representation is minimal. For example, until the 2021 national census, the number of veterans in Australia was unknown.23 In the United States (US), veterans from the Veteran Affairs system, who make up only half of the veteran population, are overrepresented in research.24
The current scoping review aims to systematically map the methodological approaches used to study the relationship between social variables and the MCT in veteran populations. In scope are recruitment strategies, data collection methods, measures and conceptual frameworks used to describe the social aspect of MCT. A secondary aim is to evaluate the quality of the methodological designs and measures used. This may enable comparison and synthesis of research findings. Importantly, it will highlight methodological strengths and trends in the literature to date and inform future research on social interventions that support veterans’ MCT.
Method
Search strategy
This scoping review followed the Joanna Briggs Institute (JBI) framework for scoping reviews25 and is reported in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR26). Searches were conducted on 28 April, 2025, across five electronic databases: APA PsycINFO, CINAHL Complete, MEDLINE Complete, Web of Science and Scopus, with no date restrictions. Key concepts searched were ‘veterans’, ‘social support’ and the ‘military-to-civilian transition’ in the titles and abstracts of articles from each database. The search terms for each concept were combined using the Boolean operator ‘AND’. The complete search strategy for the included databases is presented in Table 1.
Table 1
Complete search strategy
| Concepts | Title and abstract terms |
|---|---|
| Veterans | ‘veteran*’ OR ‘ex-service*’ OR ‘postdeployment’ OR ‘ex-military’ OR ‘discharged military’ OR ‘demobili?ed military’ OR ‘former military’ OR ‘service leavers’) |
| AND | |
| Social support | ‘social connect*’ OR ‘reconnection’ OR ‘social ident*’ OR ‘social inclusion’ OR ‘social capital’ OR ‘social integration’ OR ‘psychosocial*’ OR ‘social determinant*’ OR ‘peer support’ OR ‘community integration’ OR ‘community involvement’ OR ‘community engagement’ OR ‘social adjustment’ OR ‘social engagement’ OR ‘social support’ OR “social network*’ OR ‘social parti*’ OR ‘social change’ OR ‘belonging’ OR ‘social isolation’ OR ‘lonel*’ |
| AND | |
| Military-to-civilian transition | ‘reintegrat*’ OR ‘transition*’ OR ‘*adjust*’ OR ‘integrat*’ OR ‘adapt*’ OR ‘transitioning to civilian life’ OR ‘military?to?civilian transition’ OR ‘MCT’ OR ‘life changes*’ OR ‘Military-Civilian Transition’ |
Note. TI and AB were changed to TITLE and ABS in Scopus and TI = and AB = in Web of Science to fit database search requirements.
Inclusion and exclusion criteria
There were no inclusion criteria regarding research design, allowing for quantitative, qualitative or mixed-methods approaches. Studies were included if they met the following criteria:
(a) used veteran populations;
(b) examined both the MCT and the concept of social support;
(c) conceptualised MCT, by identifying and measuring either subjective experiences or measurable outcomes associated with leaving military service and adapting to civilian life;
(d) assessed social support either directly or through related constructs such as social connectedness, social identity, social engagement, sense of belonging, peer support or community participation, or through antithetical constructs such as social isolation or loneliness;
(e) were published in English in peer-reviewed journals.
Studies were excluded if they met any of the following criteria:
(a) Only included active-duty military personnel, non-military populations or family members of veterans.
(b) Examined non-military transitions (e.g. nursing homes, hospitals, prisons, homeless shelters or rehabilitation centres).
(c) Investigated social support solely as a therapeutic intervention for specific mental health conditions (e.g. PTSD, traumatic brain injuries (TBI)) without reference to the broader MCT process.
(d) Did not include exploration or measures of both social support and the MCT.
(e) Were classified as grey literature (e.g. dissertations or theses).
Study selection
All identified citations were imported into Rayyan, a systematic review screening software27 and duplicate records were removed. Two reviewers independently screened the titles and abstracts of all identified studies against the inclusion and exclusion criteria. Full-text screening of articles that appeared to meet the inclusion criteria was then conducted to confirm eligibility. Any discrepancies between reviewers that arose during the title/abstract or full-text screening phases were resolved by consensus prior to final inclusion or exclusion of studies.
Data charting
Key information from the included studies was extracted into a structured spreadsheet. The following data items were extracted, including article characteristics (e.g. author, title, journal, country of origin), sample characteristics (e.g. sample size, gender distribution, mean age, age range, length of military service and time since leaving military service), methodological details, including research designs, recruitment strategies, data collection methods and quantitative measures used to assess social support and the MCT. For studies that included both eligible and ineligible participants (e.g. veterans and non-veteran family members), only data from eligible participants were extracted.
Critical appraisal of individual sources of evidence
Consistent with scoping review methodology, a formal critical appraisal of study quality or risk of bias was not performed. Due to the paucity of research in this area, the goal of this review was to broadly map methodological approaches and measures in order to guide future research directions. This approach aligns with the recommended practice for scoping reviews, which aims to provide an overview of the breadth and nature of the literature and identify research gaps.28,29
Results
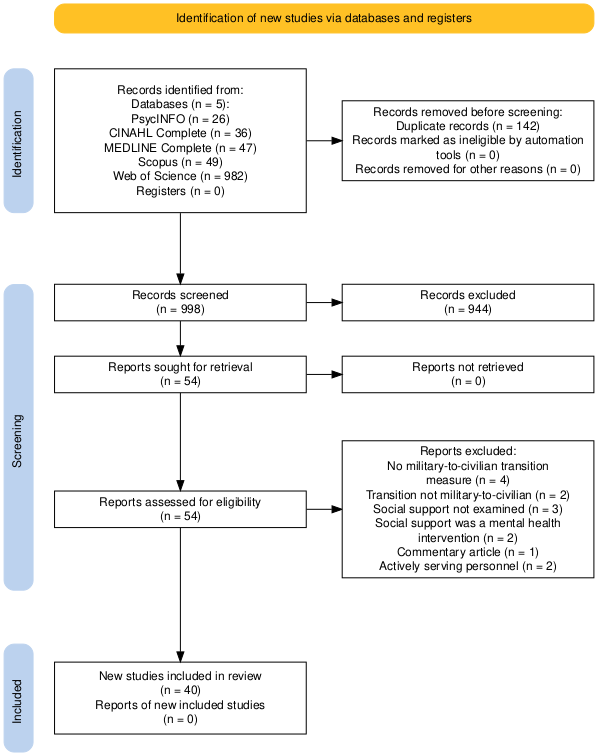
The search and selection process is presented in the PRISMA flowchart in Figure 1.30 The initial search yielded 1140 studies across the five databases. After removal of duplicates, 998 titles and abstracts were screened. Of these articles, 54 studies met the eligibility criteria and were retrieved for full-text screening. A further 14 studies were excluded, leaving 40 studies for the final review. Table 2 presents data for all quantitative studies, and Table 3 presents data for all qualitative studies included in the current scoping review.
Study characteristics
The majority of studies were conducted in the US (n = 27), followed by the UK (n = 5), Australia (n = 3) and one study each from South Africa, India, Ethiopia, Canada and Ukraine. The included studies were published between 2000 and 2025, with 38 of 40 studies published within the last 15 years. Qualitative studies were the most common research design (n = 25), followed by quantitative studies (n = 14) and a single mixed-method study.31 Sample sizes varied widely: 18 studies had relatively small samples of 3–20 participants, and 14 studies had samples larger than 100. The gender composition ranged from exclusively male veterans (n = 5) to exclusively female veterans (n = 4); 25 studies included both genders and six studies did not report gender statistics. On average, approximately 27.7% of participants across studies were women. Participants’ ages ranged from 18 to 96 years.
Military background and transition context
As seen in Tables 2 and 3, 30 studies explicitly reported the military branches of their veteran participants. Veterans came from five distinct military organisations, including the Army, Navy, Air Force, Marines and Coast Guard. One study included former members of a non-state military group, the Tigrayan People’s Liberation Front.32 Fifteen studies focused on transitions from military service to academic settings (e.g. college or university), and two studies examined transitions into civilian employment.33,34 Sixteen studies reported data on either length of military service or time since leaving service. Length of military service, when reported, ranged from 1–39 years and time since discharge ranged from 4 months to 48 years. Fourteen studies included veterans who had served in the Iraq and Afghanistan conflicts, followed by other deployments including the Vietnam War, World War II, the Gulf and Korean Wars,35 the Ethiopian Civil War,32 the East Timor conflict36 and the Russo–Ukrainian Conflict.33
Recruitment strategies
Of the 40 studies, most recruited participants from tertiary level academic institutions (n = 15), followed by veteran organisations and events (n = 7), researchers’ personal or professional networks (n = 3), military institutions (n = 2), extensive veteran population surveys (n = 3) and community settings (n = 3). Demers (2013) and Dobson et al. (2023) recruited from multiple locations, including universities, coffee houses and veteran-affiliated organisations. Five studies had unclear or unreported recruitment strategies.
As shown in Tables 2 and 3, six distinct sampling approaches were identified: purposive (n = 5), convenience (n = 2), snowball (n = 4), purposive and snowball (n = 4) and convenience and snowball sampling (n = 3). Two studies used previously collected datasets.19,35 Probability sampling was identified in three studies, including stratified random sampling,37 stratified systematic random sampling38 and random national sampling.39 However, 17 studies did not clearly report an explicit sampling strategy.
Data collection methods
In qualitative studies, semi-structured interviews were the most commonly reported method, appearing in 15 studies (see Table 2). Three studies included mixed data collection methods, with one study incorporating mapping tasks with semi-structured interviews18 and two studies combining semi-structured interviews with focus groups.40,41 Two studies used focus groups as a primary method.42,43 Additional qualitative data collection methods included photovoice, a structured interview, a life history interview, a brief five-minute interview, a case study and a qualitative self-report survey each used in a single study.19,34,44-47
In quantitative and mixed-methods studies, online surveys were the most common data collection method (n = 9) (see Table 3). Paper-based or mailed surveys were used in three studies,6,35,48 and pre-/post-surveys were reported in two studies.49,50 One study did not report the data collection method.33 One study used a mixed-methods design combining semi-structured interviews with an online survey.31
Table 2
Summary of included qualitative studies
| Author (Year), Country | Sample size (% female) | Military branch | Service length (y) | Time since military service | Age Range (y) | Military deployment | Transition type (military-to-civilian / academic / employment) | Recruitment | Methods |
|---|---|---|---|---|---|---|---|---|---|
| Ahern et al. (2015), USA | N = 24 (30) | Army; Navy; Air Force; Marines | NR | 30% of participants <1 y | 22–55 | Iraq and Afghanistan, 2009–2011 | Civilian | Advertisements to Californian veterans through organisations and events | Semi-structured interviews |
| Albertson (2019), UK | N = 35 (NR) | Army; Navy; Air Force | M = 23 | 8–43 y | 35–70 | NR | Civilian | Participant dataset in a previous two-year service program evaluation | Life history interviews |
| Barnett et al. (2022), Australia | N = 40 (15) | Army; Navy; Air Force | M = 15.1 | M = 3.3 y, | 25–57 | NR | Civilian | Advertisements through social media and veterans’ support organisations | Semi-structured interviews and two mapping tasks—social identity map and life course map |
| Binks & Cambridge (2018), UK | N = 7 (14.3) | Army; Navy | 3–24 | 1–38 y | 38–58 | NR | Civilian | Purposive or snowball sampling of veterans known to researchers | Semi-structured interviews |
| Blauuw-Hara (2016), USA | N = 6 (0) | Army; Navy; Air Force; Coast Guard | NR | NR | 25–45 | NR | Academic | Word of mouth and flyers for student veterans at a rural community college | Semi-structured interviews |
| Demers (2013), USA | N = 17 (100) | Army; Navy; Marines | NR | NR | 22–43 | Iraq and Afghanistan | Civilian | Purposive sampling of female Iraq War veterans around San Francisco, California, through online advertisements, flyers at universities, coffee houses and veteran organisations and word of mouth through veteran-affiliated groups | Focus groups |
| Dobson et al. (2023), USA | N = 7 (0) | Army; Navy; Marines | NR | NR | 22–30 | NR | Academic | Via flyers, email and in-person recruitment of student veterans at the University of Wisconsin-Milwaukee (UWM) | Photovoice |
| Gorman et al. (2018), USA | NRa | NR | NR | NR | NR | NR | Civilian | Peer specialists partnered with clinical teams to form local veteran peer support groups in community locations across Massachusetts. | Case descriptions of specific group and attendees from case study data over nine months |
| Gregg et al. (2016), USA | N = 13 (15) | Army; Marines; Air Force | NR | NR | 22–32 | NR | Academic | Purposive a sampling of student veterans comparable to the active military population and additional snowball sampling via flyers and emails | Semi-structured interviews |
| Gregg et al. (2018), USA | N = 12 (24) | Army; Navy; Air Force; Marines | NR | NR | 22–42 | Iraq and Afghanistan | Academic | Purposive sampling of student veterans with flyers and emails at two public universities | Semi-structure interviews |
| Guthrie-Gower & Wilson-Menzfeld (2022), UK | N = 11 (45.5) | Army; Navy; Air Force | M = 19 | M = 20 y | 49–72 | NR | Civilian | Voluntary and snowballing sampling through researcher’s professional network by email and social media | Semi-structured interviews |
| Jones (2017), USA | N = 5 (20) | Army; Marines | NR | NR | 26–mid-40s | Iraq and Afghanistan | Academic | Purposive criterion sampling of student veterans from a Florida community college | Semi-structured interviews |
| Kato et al. (2016), USA | N = 19 (21.1) | Army; Navy; Air Force; Marines | NR | NR | 23–46 | Iraq and Afghanistan | Academic | Convenience and snowball sampling of student veterans from a community college in Southern California via flyers | Semi-structured interviews |
| Killam & Degges-White (2018), USA | N = 15 (0) | Army | NR | NR | 25–46 | NR | Academic | Flyers on academic campus | Structured interviews |
| Kramm & Heinecken (2015), South Africa | N = 14 (21.4) | South African National Defence Force (SANDF) | NR | NR | 21–28 | NR | Civilian | Convenience and snowball sampling by a South African Infantry School commander | Semi-structured interviews and focus groups |
| Leslie & Koblinsky (2017), USA | N = 29 (100) | Army; Navy; Air Force; Marines | NR | NR | 26–56+ | Iraq and Afghanistan | Civilian | Convenience sampling by non-profit veteran organisations in the mid-Atlantic region via email | Focus groups |
| Mahoney et al. (2023), USA | N = 12 (8.3) | Army; Air Force; Marines | NR | 4–32 y | 23–58 | NR | Academic | Purposive sampling of student veterans at universities around the Rocky Mountain region via email | Semi-structured interviews |
| Mayer et al. (2023), USA | N = 20 (NR) | NR | NR | <1 y | NR | NR | Academic | Recruited by military program directors at the University of South Carolina Beaufort and the Lowcountry Veterans’ Centre | Semi-structured interviews |
| Miller & Saling (2024), Australia | N = 10 (50) | Army; Navy; Air Force | 1–30 | 4 mth–24 y | 33–61 | Afghanistan, Middle East, East Timor | Civilian | Purposive sampling of post-1990 Australian Defence Force veterans via social media and a veteran support organisation | Semi-structured interviews |
| Negewo-Oda & White (2011), Ethiopia | N = 20 (100) | Ethiopian Women Veterans from the Tigray People’s Liberation Front | NR | NR | 36–55 | Ethiopian Civil War | Civilian | Snowball sampling of former Tigray People’s Liberation Front women veterans | Semi-structured interviews |
| Rattray et al. (2024), USA | N = 44 (13.6) | Army; Navy; Air Force; Marines | NR | M = 1.7 y | 21–53 | NR | Civilian | Convenience sampling of veterans who attended outreach events in Indiana | Brief five-minute interview |
| Roy et al. (2020), Northern Ireland, UK | N = 252 (11) | Army; Navy; Marines; Air Force | NR | M = 21 y | 25–65+ | NR | Employment | Via social media, newspaper advertising, local charities and veteran organisations | Online and paper self-report survey |
| Sharma & Hussain (2025), India | N = 17 (0) | Army; Navy; Air Force | 20–39 | 2–33 y | 57–87 | NR | Civilian | Recruited commissioned officers from the army, navy and air force | Semi-structured interviews |
| Shue et al. (2021), USA | N = 15 (26.7) | Army; Navy; Air Force; Marines; Coast Guard | M = 9.4 | M = 8.3 mth | 18–54 | Iraq and Afghanistan | Civilian | Purposive and snowball sampling and word of mouth from veteran organisations and university veteran service departments | Semi-structured interviews |
| Wakefield et al. (2024b), UK | N = 14 (28.6) | Army; Navy; Air Force | 5–28 | 10 mth–48 y | 28–77 | NR | Civilian | NR | Semi-structured interviews |
| Yeager & Rennie (2021), USA | N = 12 (33.3) | Army; Navy; Air Force; Marines | NR | NR | 23–30 | NR | Academic | Student veterans via flyers and social media | Semi-structured interviews and focus groups using photovoice |
Note. M = mean; NR = Not reported. The Coast Guard is considered a military branch in the United States.
Gorman et al. (2018) reported total number of engagements, not number of participants. b Wakefield et al. (2023) was a mixed-methods research design with the qualitative component (Study 2) reported in the above table.
Measures and conceptual frameworks for social support
As shown in Table 3, there were 15 distinct measures for social support. The Medical Outcomes Study Social Support Survey (MOS-SSS),51 which assessed social support, was the most commonly used, appearing in three studies.35,39,50 All other studies used distinct measures of social support (see Table 3). Reported internal consistency ranged from 0.70 to 0.98. (see Table 3). A test-retest reliability of 0.85 was reported for the Multidimensional Scale of Perceived Social Support52 in one study.53 Two studies had custom measures and did not report any validity or reliability coefficients.49,54 Four dedicated conceptual frameworks were identified, including the Social Identity Approach,55 the Social Identity Model of Identity Change (SIMIC),56 Sense of Community Framework (SOC)57 and Cultural Incongruity.58
Measures and conceptual frameworks for the military-to-civilian transition
As shown in Table 3, 17 distinct measures for MCT were identified. The most commonly used MCT measure was the Military-to-Civilian Questionnaire (M2C-Q),37 which was used in three studies.48-50 The Student Adaptation to College Questionnaire (SACQ)59 was used in two studies to assess transition to tertiary education.22,53 Two studies31,60 evaluated the MCT using the Satisfaction with Life Scale (SWLS).61 All other measures were distinct and were only reported for their individual studies. Reported internal consistency for the included measures ranged from 0.64 to 0.95. A test-retest reliability of 0.82 was reported for the Satisfaction with Life Scale52 in one study.60 Two dedicated MCT theoretical frameworks were identified, the Social Identity Model of Adjustment to Identity Change56 and the Military Transition Theory.62
Table 3
Summary of included quantitative studies
| Author (Year), Country | Sample size (% female) | Military branch | Service length (y) | Time since military service | Age Range (y) | Military deployment | Transition type (military-to-civilian / academic / employment) | Recruitment | Methods | Theory for social support | Measure for social support | Theory for MCT | Measure for MCT |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baird et al., (2018a) USA | N = 60 (NR) |
NR | NR | NR | NR | Iraq and Afghanistan | Civilian | Recruited from multiple cities via social media and veteran events | Experimental study with between-subjects design, pre/post surveys | NR | Team RWB Enriched Life Scale (ELS) | NR | Military to Civilian Questionnaire (M2C-Q),36 Cronbach’s α = 0.95 |
| Campbell & Riggs (2015), USA | N = 117 (16.2) | Army; Navy; Air Force; Marines | NR | NR | 21–53 | Iraq and Afghanistan | Academic | Student veterans via email at a Texas university | Online survey | Social Support | Multidimensional Scale of Perceived Social Support (MSPSS),51 r = 0.85, α =0.89. | Adjustment to college | Student Adaptation to College Questionnaire (SACQ),58 α = 0.90 |
| Cotten et al. (2000), USA | N = 2121 (100) | NR | NR | NR | 20–95 | World War II, Korean War, Vietnam War, Post-Vietnam, Persian Gulf | Civilian | Drawn from national sample of women veterans who have used VA ambulatory care | Self-administered mailed surveys | Social support, loneliness and social functioning | Five items from Medical Outcomes Study (MOS50) Social support survey, α = 0.90 |
Strains relating to lived experience, e.g. problems with relatives, finance, housing | Self-made questionnaire -four items for living strains, three items for loneliness, two items for social functioning from Medical Outcomes Study (MOS) Short-form 36-Item Health Survey, (SF-36),86 α = 0.86 |
| Eakman et al. (2019), USA | N = 162 (17) | NR | NR | NR | 20–59 | Iraq and Afghanistan | Academic | Student veterans through Colorado State University’s veteran services. | Online survey | Social Support | Post-deployment Support Questionnaire | Community Participation | Veterans’ Social and Community Participation Assessment |
| Flack & Kite (2021), Australia | N = 358 (31) | Army; Navy; Air Force | M = 14 | NR | 20–66 | NR | Civilian | Convenience and snowball sampling via social media and researchers’ veteran networks | Online survey | Social Identity Approach | Social connectedness scale-revised (SCS-R)101 α = 0.96 | Social identity model of adjustment to identity change Military Transition Theory |
WHO Quality of Life Bref (WHOQOL-Bref) scale, α = 0.76–0.90, Kessler psychological distress scale (K-10),102 α = 0.95 |
| Geraci et al. (2023), USA | N = 200 (16) | Army; Navy; Air Force; Marines | NR | M = 2.77 y | 20–40+ | NR | Civilian | Recruited New York veterans via flyers | Experimental study with between-subjects design, pre/post surveys | NR | Medical Outcomes Study Social Support Survey,50 α = 0.98. |
NR | Military to Civilian Questionnaire (M2C-Q),36 α = 0.95 |
| Kolenichenko et al. (2021), Ukraine | N = 512 NR | NR | NR | NR | 20–36+ | Russo-Ukrainian Conflict 2010–2021 | Employment | NR | NR | Social Reintegration | Post-deployment Social Support, α = 0.98. |
Employment | Employment—questions about employment status |
| Lee et al. (2023), Canada | N = 595 (12) | Army; Navy; Air Force | 2–35+ | NR | 20–50+ | Afghanistan | Civilian | Stratified systematic random sampling from larger Canadian Armed Forces veteran survey | Online survey | Social support | Social Provisions Scale-10 (SPS-10), α = 0.94 |
Perceived transition challenges | Perceived transition challenges survey, α = 0.64 |
| McAndrew et al. (2019), USA | N = 814 (30.1) | NR | NR | NR | 18–84 | NR | Academic | Snowball sampling of student veterans via email through the Student Veterans of America (SVA) organisation | Online survey | Cultural incongruity Social support |
Cultural Congruity Scale, α = 0.90 Social support—Patient-Reported Outcomes Measurement Information System (PROMIS) short form v2.0 Emotional Support 4a scale, α = 0.96 |
Adjustment to College | Student Adaptation to College Questionnaire (SACQ),58 α = 0.95 |
| Sayer et al. (2010), USA | N = 754 (13) | NR | NR | NR | 22–62 | Iraq and Afghanistan | Civilian | Stratified random sampling without replacement of combat veterans who made at least one visit to a VA facility | Paper questionnaire | Social relationships | Eight items for social relations and functioning from the WHO Disability Assessment Schedule II,107 α = .95 | NR | Items from the WHO Disability Assessment Schedule II Community Integration Questionnaire and Community Integration Measure |
| Smith et al. (2017), USA | N = 61 NR | NR | NR | NR | NR | NR | Academic | Via email to all undergraduate students at a community college and two Catholic colleges in Pennsylvania, New Jersey and New York | Online survey | NR | Social engagement domain of the questionnaire, α = 0.85 | NR | Fitting In domain of the questionnaire, α = 0.85 |
| Thomas & Bowie (2016), USA | N = 131 (6.1) | NR | NR | NR | 21–75 | Iraq and Afghanistan, Gulf War, Cold War, Vietnam | Civilian | Recruitment: Purposive sampling of veterans at a career fair in the southern US | Paper survey | Sense of Community Framework | Brief Sense of Community scale (BSCS),110 α = 0.92 | Community reintegration | Military to Civilian Questionnaire (M2C-Q),36 α = 0.95 |
| Umucu et al. (2023), USA | N = 205 (27.8) | Army; Navy; Air Force; Marines; Coast Guard | NR | NR | 18–64 | NR | Academic | Student veterans recruited through veteran student services programs at multiple colleges and universities via email | Online survey | Social support | Oslo Social Support Scale (OSSS-3), α = 0.70 | Subjective Wellbeing | Perceived Stress Scale-4 (PSS-4), α = 0.74 Satisfaction with Life scale (SWLS) α = 0.90, r = 0.82 |
| Wakefield et al. (2024b), UK | N = 210 (22) | NR | NR | NR | 19–88 | NR | Civilian | NR | Online survey | The Social Identity Model of Identity Change | Exeter Identity Transition Scale, α = 0.90–0.95 |
Loneliness, Subjective Wellbeing | UCLA Loneliness Scale114 Psychological Resources via Meaning in Life Questionnaire—Short-form.115,116 α = 0.94 Life satisfaction scale, α = 0.93 Depression scale (DASS 14), α = 0.93 |
| Weiner et al. (2016), USA | N = 290 (0) younger veterans, 326 (0) older veterans | Army; Navy; Air Force; Marines | NR | NR | 21–46 78–96 |
NR | Civilian | Random national sampling with data from the National Health and Resilience in Veterans Survey |
Online survey | Social Support | Medical Outcomes Study Social Support scale,50 α = 0.91 One item for number of close friends and relatives |
Community reintegration | Single item—‘I feel well-integrated in my community.” |
Note. M = mean; NR = Not reported. The Coast Guard is considered a military branch in the United States.
Baird et al. (2018) presented a study protocol, outlining the research methodology. b Wakefield et al. (2023) was a mixed-methods research design with the quantitative component (Study 1) reported in the above table.
Discussion
This scoping review aimed to map the methodological approaches and measures used to study the relationship between social support and the MCT. Forty peer-reviewed studies were included: 25 qualitative studies, 14 quantitative studies and one mixed-methods study, for a total sample of 7586 veterans. The large proportion of qualitative research (62.5%) suggests that the field is in an exploratory phase. Our findings reveal substantial heterogeneity in research design, recruitment strategy, data collection methods, measures and conceptual frameworks.
Study characteristics
Over the past 25 years, research on social support and the MCT has grown significantly. Only seven of the included studies were published before 2015, while 32 were published between 2015 and 2025—nearly a fivefold increase, indicating a rapidly developing body of literature. Participants were primarily from Western countries, with over two-thirds of studies conducted in the US (n = 27). This concentration reflects a considerable population bias towards US veterans. Cross-national research indicates that Americans report consistently higher levels of loneliness than peers in European countries63 and US veterans have a greater prevalence of PTSD than comparably deployed UK veterans.64 Therefore, findings from US-based veterans may be less generalisable to global veteran populations, particularly to veterans outside Western cultural contexts.
Most studies (n = 25) included both male and female veterans, with four studies focusing exclusively on women.32,35,42,43 Research on female veterans is an emerging priority as the number of women in the military grows65,66 and women may face distinct MCT challenges, such as accessing gender-sensitive healthcare services, conflict between expected civilian feminine norms with military norms and experiencing sexual discrimination, harassment or assault during military service.67,68 Female veterans have reported higher incidences of military sexual trauma, higher risks of underdiagnosed PTSD and disconnection from non-veteran women.68-70 Given only a few studies focused exclusively on female veterans, gender-specific transition challenges are likely underrepresented in the literature.
More research on female veterans is required to establish if there are gender differences in the relationship between social support and the MCT process.
Participants across studies varied in service branch, length of service and time since military discharge. Most studies that reported military deployment sampled post-9/11 veterans, e.g. Iraq and Afghanistan veterans (n = 14). This focus on post-9/11 veterans may be attributed to the recent growth in MCT research, which has enabled the recruitment of veterans from more recent conflicts. Military service length ranged from 1 to 39 years, and time since military discharge ranged from 4 months to 48 years. Some studies examined short-term transitions (e.g. within 1–2 years20,47,71), while others included veterans who had transitioned decades earlier.31 This variation suggests that MCT experiences may differ significantly depending on service era and time since transition. This is consistent with research indicating that younger, more junior military personnel who had transitioned recently reported the most difficult transitions.72 However, over half of the studies (n = 25) did not report these variables. Future research should consistently report service history to enable assessment of whether differences in length of service and time since discharge affect the continuity of social support.
Recruitment strategies
This scoping review revealed substantial heterogeneity in recruitment strategies. Academic institutions were the most common recruitment location, with 15 studies (37.5%) recruiting US student veterans transitioning to universities, community colleges or student veteran organisations. This research focuses on US student veterans, and may be attributed to the availability of education benefits, e.g. the Post-9/11 GI Bill, which incentivises military personnel to pursue tertiary education after military service.73 Approximately 73% of separating service members report plans to use such benefits, making student veterans an easily accessible population for researchers.74 However, college-based veteran populations may not reflect the broader military demographics.75 Veteran-affiliated organisations were also a common recruitment setting. While a broad age range of participants was sampled (22 to over 56 years old),43,71 many studies did not report mean age. Given prior research highlighting individuals affiliated with veteran services organisations are more likely to be older and retired,76 the transition experiences of older veterans may be disproportionately reflected in studies using this recruitment strategy.
These recruitment approaches raise several methodological limitations concerning representativeness. A key limitation was sampling bias, as participants were mainly recruited from veteran support organisations. However, these populations may be unrepresentative of the general veteran population, as research suggests that between 32–55% of veterans do not seek support services for mental or physical health problems.77-79 Therefore, recruitment from predominantly academic and veteran organisations may result in an overrepresentation of socially connected veterans, while underrepresenting specific veteran populations, including socially disengaged veterans, younger veterans not pursuing higher education and veterans transitioning into workplace settings. Future research should investigate these potential populations to better represent the experiences of transitioning veterans across the full spectrum.
Non-probabilistic sampling methods, such as convenience, snowball and purposive sampling, were the most commonly used and were explicitly reported in half of the included studies. However, 17 studies (42.5%) did not clearly report their sampling strategy, underscoring the need for greater methodological transparency. Transparent reporting of recruitment and sampling methods is essential for improving study replicability and evaluating the trustworthiness and external validity of research findings.80,81 Furthermore, a lack of explicit reporting of the sampling strategy undermines the ability to evaluate whether sample demographics are representative of the general veteran population and enables replicability of studies.
Data collection methods
There was considerable diversity in data collection methods. Qualitative data collection methods (n = 25) were the most common, including semi-structured interviews (n = 15) and focus groups (n = 2) used independently (see Table 2). Semi-structured interviews facilitated in-depth exploration of participants’ lived experiences, but limitations included the risk of response bias stemming from the interviewer’s demeanour or skill.82,83 In comparison, focus groups were beneficial in encouraging interactive discussion and generating ideas beyond individual interviews.42
For quantitative data collection methods, online surveys were the most common (n = 9). However, there was a relative lack of experimental or longitudinal designs using pre-/post-surveys (see Table 3). Previous longitudinal studies have demonstrated that social support is a protective factor for depressive symptoms, suicidal ideation and loneliness during transitional life periods such as adolescence.84,85 However, as most quantitative studies were cross-sectional, they were unable to determine if social support demonstrated similar effects during the MCT. More quantitative research, including longitudinal research, is needed to assess whether social support has a causal relationship with successful MCT outcomes.
Measures and conceptual frameworks for social support and the MCT
There was substantial variation in the measures for social support and the MCT. Fifteen distinct measures for social support and 17 distinct measures for the MCT were identified. The most frequently used measure of social support was the Medical Outcomes Study Social Support Survey (MOS-SSS),51 and the most frequently used MCT measures were the Military-to-Civilian Questionnaire (M2C-Q)37 and the Student Adaptation to College Questionnaire (SACQ)59 for the transition to academic environments.
However, several limitations were noted in the measures selected. While the majority of social support and MCT measures reported strong psychometric properties such as high internal consistency (α ≥ 0.80), only a limited number had been explicitly validated with veteran populations. These included the Post-deployment Social Support scale,86 the Military-to-Civilian Questionnaire (M2C-Q),37 the SF-36,87 and the WHOQOL-Bref scale88 for MCT-related outcomes. This is a significant limitation, as veteran cohort characteristics may differ substantially from those of the general population. For example, veterans experience significantly higher rates of PTSD compared to the general population, with prevalence estimates ranging from 12% to 50%.89 Hence, using non-validated measures for veteran populations risks underrepresenting the prevalence of transition-related difficulties such as PTSD and social isolation. Subsequently, general psychosocial functioning measures used to assess the MCT may not comprehensively capture key aspects of the MCT, such as post-deployment stressors, sense of belonging or connection to other people.37 As a result, non-validated measures may lack content validity, resulting in less comprehensive measurement of the MCT. Further research is required to validate measures of social support and MCT that are specifically tailored to veteran populations, enabling accurate and early identification of vulnerable veterans at heightened risk of reintegration difficulties.
A further limitation was the lack of measures that were selected based on conceptual frameworks. Of the 40 studies reviewed, only four social support measures were explicitly grounded in theoretical frameworks. These measures drew on conceptual frameworks such as the Social Identity Approach,55 the Social Identity Model of Identity Change,56 the Sense of Community Framework (SOC)57 and Cultural Incongruity.58 Similarly, among MCT measures, only one, the WHO Quality of Life-BREF (WHOQOL),90 was associated with dedicated conceptual frameworks, drawing from the Social Identity Model of Adjustment to Identity Change56 and the Military Transition Theory.62 The absence of clearly defined conceptual frameworks suggests that measure selection was often conducted in an ad hoc manner. This is a methodological concern, as the lack of conceptual frameworks can lead to poor operationalisation and to the selection of measures that do not fully capture the examined construct.91 For example, one study only used a single-item question for community reintegration to represent the MCT.39 As a result, key aspects of the transition, such as identity change or cultural adjustment, may be underrepresented.11 Furthermore, the absence of theory-driven measures also contributes to the inconsistent operationalisation of social support and the MCT across studies, which can limit the comparability and synthesis of findings.92 Future research should incorporate theory-driven frameworks to guide measure selection, thereby improving the validity and accuracy of measures that can be applied to veteran research and assessment of veterans in clinical settings.
Limitations of the current review
Although multiple databases were searched, including multidisciplinary databases, additional literature available only in defence or veteran-specific journals may have been overlooked. Non-English-language studies were also excluded due to translation limitations, potentially contributing to a bias towards English-speaking veterans. Consequently, specific veteran populations may have been underrepresented in this review.
Suggestions for future research
Several methodological recommendations are proposed for future research to address key gaps in sample representation, methodological transparency, research design and measurement tools. Given the underrepresentation of certain veteran populations in the current literature, future research should prioritise recruiting veterans from diverse backgrounds, including greater representation of women, younger veterans not pursuing higher education, socially isolated veterans and veterans transitioning to employment settings. Moreover, more research on non-US veterans is recommended. By doing so, this will help identify whether there are specific differences in social support during the MCT across various veteran subgroups and improve the generalisability of findings to the general veteran population. In addition, this review highlights the need for greater methodological transparency, particularly through more consistent reporting of sampling strategies and relevant demographic variables such as length of military service and time since transition. This will enable better evaluation of sampling bias, improve study replicability and clarify whether these variables are relevant predictors of reintegration difficulty. Further work is also needed for more longitudinal and experimental designs to examine causal relationships between social support and the MCT. Finally, there is a need for the development and validation of veteran-specific measures grounded in clear theoretical frameworks, which would improve construct validity and ensure vulnerable veterans, such as those with PTSD or experiencing social isolation, are accurately identified and supported.
Conclusion
The current scoping review mapped the methodological approaches and measures used in 40 peer-reviewed studies examining the relationship between social support and the MCT. These findings suggest that the research field is in an exploratory stage, with considerable heterogeneity in recruitment strategies, data collection methods, quantitative measures and underlying conceptual frameworks. An important next step for researchers is to improve methodological rigour by increasing the representation of diverse veteran populations, using more experimental and longitudinal designs, improving transparency in reporting and developing validated, veteran-specific measures. This review implies that these improvements will contribute to a more coherent and robust empirical foundation for applied practice and research. Furthermore, the development of a stronger evidence base can guide future research into effective, tailored psychosocial interventions that integrate social support to support successful MCTs for veterans. Correspondingly, the development of valid veteran-specific measures will improve screening and early identification of veterans at risk of social isolation during the MCT, enabling earlier support and care.
Funding
This study was not supported by any funding
Please specify the URL of your file